 作者投稿
作者投稿 专家审稿
专家审稿 编辑办公
编辑办公 邮件订阅
邮件订阅 RSS
RSS
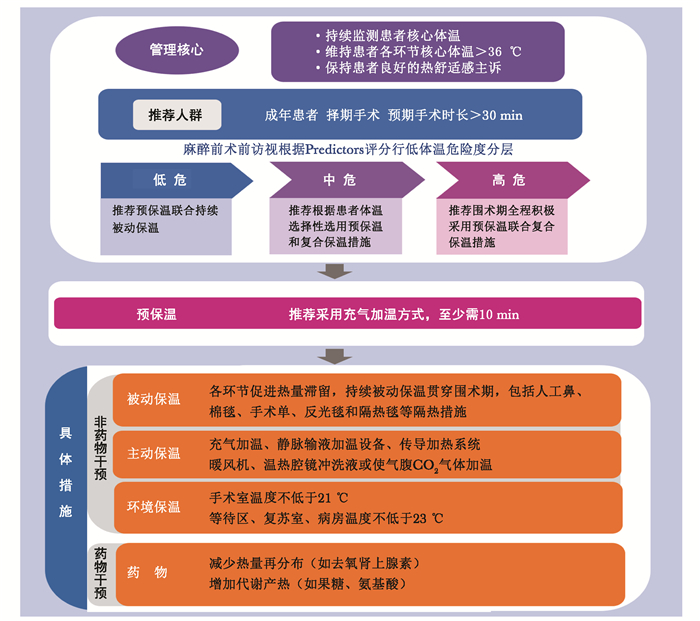
围术期患者低体温防治专家共识(2023版)
详细信息2023 Chinese Expert Consensus Statement for Prevention and Management of Perioperative Hypothermia
-
摘要: 《围术期患者低体温防治专家共识(2023版)》在《围手术期患者低体温防治专家共识(2017)》基础上进行更新。新版共识旨在以患者为中心,以防治围术期意外低体温为目的,为临床医生提供实现优质医疗服务的循证医学证据与建议。该共识对围术期低体温风险评估与预测、常用的体温监测方法以及在术前、术中和术后为患者提供保温措施等方面提出专业建议。此外,共识还对低体温与不良结局,儿科、妊娠、创伤、肝移植和败血症等特殊患者体温管理提供了新的证据。Abstract: The 2023 Chinese Expert Consensus Statement for Prevention and Management of Perioperative Hypothermia is an update of the 2017 Chinese Expert Consensus Statement for Prevention and Management of Perioperative Hypothermia. It is intended to provide patient-centric recommendations for clinicians to prevent and manage inadvertent hypothermia. It offers advice on assessing patient's risk of hypothermia, measuring and monitoring temperature as well as preventing patients from hypothermia before, during and after surgery. It also provides new evidence on hypothermia and adverse outcomes, and temprature management for special patients care considerations including pediatric, pregnancy, trauma, liver transplantation and sepsis.
-
Keywords:
- perioperative /
- hypothermia /
- prevention /
- management /
- expert consensus
-
术后快速康复,或加速康复外科(enhanced recovery after surgery,ERAS)近年来日益受到外科医生和护理人员的关注。ERAS的理念强调,通过术前咨询、避免术前灌肠、术中使用局部麻醉、术后早期进食、避免过多静脉补液、减少不必要引流管放置等措施可减轻手术应激,加速术后恢复,降低手术并发症和医疗费用[1-2]。ERAS在妇科手术中对住院天数、术后疼痛等临床结局的改善作用已经得到多中心研究的证实[3],包括产科[4]、盆底手术[5]、妇科肿瘤手术[6]、微创手术[7]。ERAS不仅具有明显的卫生经济学效益[8],患者也有较好的满意度[9]。在ERAS的理念下,产生了大量日间手术,不仅用于妇科良性疾病,还用于妇科肿瘤和盆底手术[10]。本文着重讨论妇科肿瘤手术创伤对ERAS的影响及可能的改进措施。
1. 妇科肿瘤加速康复外科指南和争论
目前已有多个妇科肿瘤ERAS指南和清单[2, 11-15],包括肿瘤手术方案[16-19],均根据不同证据级别提供相应推荐。2019年指南还新加入了患者报告结果、盆腔廓清术、盆腔热灌注、出院路径以及评估和报告等诸多新条目[11],系统性地执行和评估ERAS已成为妇科肿瘤治疗的共识[20]。妇科肿瘤ERAS项目甚至还延伸至术前患者的锻炼和康健指导[21]以及卫生经济学领域[22]。中国医师协会妇产科医师分会于2019年亦成立了专门的ERAS学组,可见对该问题的重视。
尽管如此,ERAS在妇产科手术中的应用仍有很多未知之处[23],在复杂手术治疗如妇科肿瘤手术中仍存在不同看法[24-28],特别是对卵巢癌的治疗[29-30]。研究发现,在卵巢癌治疗中,ERAS对于初始手术和中间型手术的恢复并无明显区别[25]。但系统性回顾并未得到更多有关卵巢癌手术实施ERAS的效应信息[30]。值得关注的是,在讨论ERAS的众多研究中,手术创伤对于术后康复的影响一直未得到应有的重视,这可能是目前ERAS研究中最大的悖论和矛盾,然而这方面的研究较少。在临床实践中,笔者认为减少手术创伤始终是快速康复的决定因素,如不能避免和减少预期或计划外手术创伤,ERAS的大部分举措则不仅无益,还可能产生负面效应。
2. 妇科肿瘤手术执行加速康复外科的要点
2.1 尊重学习曲线,减少研究偏倚
手术学的学习曲线是每个外科医生必须经历的过程。尽管个人天赋或能力具有差异,学习曲线或长或短,但为了达到可接受的熟练程度和安全阈值,手术医生无不需要经历一系列严格的培训。已有研究发现,不同妇科肿瘤团队施行ERAS的实践和效果具有很大的异质性[24]。因此,在施行ERAS之前,应把医生的学习曲线作为重要的变量予以考虑和平衡;在评估ERAS效果之时,应将医生的学习曲线作为重要的因素予以分层和校正[31]。而ERAS本身也有其学习曲线的问题[32],多学科合作下的ERAS对于重大肿瘤手术才能发挥有益价值[16],医生的拥护亦是ERAS实践成功的关键[33]。
良性手术以及开腹手术是目前妇产科领域ERAS研究的主要对象。在妇科恶性肿瘤手术,尤其是微创妇科肿瘤手术中对ERAS的效果仍然存在争议,究其原因还是手术的复杂性和高风险影响了ERAS的实施与效果评定[34]。微创手术有巨大的异质性,从简单的探查术、诊断术、活检术,到复杂的根治术、分期术、廓清术,手术创伤存在巨大的层级差异,复杂程度和并发症风险亦有天壤之别,这种异质性对ERAS的实施和评估必然产生重大影响[35]。因此,对于复杂手术实施ERAS的情境下,适宜在相同手术类型中进行风险比较,并充分考虑医生的学习曲线,从而减少临床研究偏倚,充分阐释ERAS的效果。如果忽略这些问题,则有可能得出过于激进或过于保守的结论,无法指导复杂多变的临床问题。
2.2 全面规划手术,规避手术风险
手术永远存在风险,实施手术永远是在利大于弊的前提下进行的决策判断。为了保证ERAS的实施,规避手术风险,消除医患矛盾,应对手术进行全面规划设计,充分考虑到所有的意外和最大的风险,这一点对任何级别的医师来说都是必备素质。尽管实施ERAS的患者满意度较高,亦需根据患者具体情况区别对待。研究发现,日间手术患者中独居或年龄较大者对术后当天出院的感受会差很多[10]。对于不同年龄和功能评分的妇科肿瘤患者,实施ERAS的安全性亦需进一步证实[36]。美国妇产科医师协会指南认为,实施ERAS前应仔细审查手术和护理框架及流程,并将ERAS植入卫生系统以获得持续效果[2]。
支持ERAS的证据很多,严密实施ERAS的好处亦很多,但ERAS的地位永远是辅助手术、以手术为中心的。不能因为ERAS而去破坏和干扰已经成熟实施、卓有成效的临床路径和方案,而应采用ERAS的理念修订、改善和弥补现有的临床路径及方案,并在修订、改善和弥补的过程中,尊重传统手术学经验,因为经验也是一种证据[37]。现有的循证医学材料和证据则应在全面规划的前提下审慎地改造、植入和运用,以避免新证据在老传统中“水土不服”,避免新事物在老环境下“夭折短命”。这种系统性工作并非一朝一夕、一人一事就能够实现的。经历6年的多中心研究已经证实,如果能够在术中和围手术期严格遵循妇科手术的ERAS指南,可改善患者的临床结局[3]。而一项德国妇科医生的调查发现,仅有1/3的被调查者会遵循ERAS相关指南[38]。很难想象,在一个管理混乱、缺乏规范准入制度的手术中心能够很好地推广和延续ERAS;即便能够强行推广,也不过是手术风险增加的导火索。
2.3 总结失利经验,开展前瞻研究
ERAS可以降低手术并发症,但不能完全消除手术并发症。除了手术学本身的机会性风险之外,手术创伤与ERAS的相关性问题目前尚未得到充分研究。这是一个非常有趣且存在巨大挑战的课题。从这样的相关性研究中,不仅可深入了解ERAS促进术后康复的机制,还可阐释手术学创伤对ERAS的效应与后果,诸如镇痛与住院时间的关系等[6, 27]。手术的失利包括未达到预期目的、严重的并发症、超出一般水平的恢复时间和花费。分析这些失利的可能因素,无论是从个体层面,还是从研究层面,都将有助于手术学和ERAS的完善与革新,有益于患者的身心健康和快速康复。
ERAS成功和失利的教训都会为临床实践提供宝贵的经验,尤其是失利的经验,对于复杂性、高风险手术而言具有更加宝贵的警示和帮助作用,为高质量的前瞻性研究提供切入点。这些内容包括:患者心理因素与生活质量的变化及其对手术预后和生存结局的影响[39];围手术期饮食与禁食应激对肠道微环境的影响[40];麻醉方式对机体免疫环境以及预后的影响[41];不同方式引流及放置时长对于术后康复的影响,等等。这些研究涉及临床、护理、病/生理和分子机制等多个方面,无论阴性结果还是阳性结果,均可为ERAS的广泛开展和个体化操作提供更多细节和更可靠的证据。
3. 结语
手术创伤永远是决定手术结局的关键因素,而减少手术创伤始终是ERAS的决定性因素,这一点在目前的ERAS研究中尚未得到充分重视,在诸如妇科肿瘤等复杂手术中尤甚。作为外科医生,我们应该尊重手术学的学习曲线,在复杂手术应用ERAS的评估中减少术者因素的偏倚。而每一个重视自己手术技巧、珍爱患者预后的术者都会因地制宜、扬长避短地全面规划手术及围手术期护理,从而规避手术风险,保证ERAS实施的有效性和可持续性。无论是手术还是ERAS的失利,都需要总结经验、及时完善和修订,并在前瞻性研究中探讨成功和失利的潜在因素,从而保证诊疗技术的全面进步,并为患者健康提供可靠保障。
作者贡献:顾小萍负责查阅文献;顾小萍、易杰、裴丽坚负责撰写初稿;黄宇光负责修改完善并审校定稿;其余成员参与修订。利益冲突:共识制订工作组所有参与人员均声明不存在利益冲突共识专家组名单组长:黄宇光(中国医学科学院北京协和医院)成员 (按姓氏首字母排序):柴小青(中国科学技术大学附属第一医院),陈骏萍(浙江省宁波市第二医院),陈世彪(南昌大学第一附属医院),迟永良(山东省中医院),都义日(内蒙古医科大学附属医院),顾小萍(南京大学医学院附属鼓楼医院),郭曲练(中南大学湘雅医院),嵇富海(苏州大学附属第一医院),李洪(陆军军医大学第二附属医院),李天佐(首都医科大学北京世纪坛医院),林献忠(福建医科大学附属第一医院),刘友坦(南方医科大学深圳医院),陆智杰(海军军医大学第三附属医院),贾珍(青海大学附属医院),马正良(南京大学医学院附属鼓楼医院),欧阳文(中南大学湘雅三医院),裴丽坚(中国医学科学院北京协和医院),田首元(山西省肿瘤医院),王庚(北京积水潭医院),王国林(天津医科大学总医院),王晟(北京安贞医院),王天龙(首都医科大学宣武医院),夏中元(湖北省人民医院),徐铭军(首都医科大学附属北京妇产医院),严敏(浙江大学医学院附属第二医院),杨建军(郑州大学第一附属医院),姚兰(北京大学国际医院),易杰(中国医学科学院北京协和医院),赵国庆(吉林大学中日联谊医院),赵平(中国医科大学附属盛京医院),章放香(贵州省人民医院),张良成(福建医科大学附属协和医院),郑晖(中国医学科学院肿瘤医院),左明章(北京医院)执笔人:顾小萍(南京大学医学院附属鼓楼医院),易杰(中国医学科学院北京协和医院),裴丽坚(中国医学科学院北京协和医院) -
表 1 围术期低体温的危险因素
因素 具体描述 患者因素 年龄 年龄>60岁的患者围术期低体温发生率更高,体温恢复时间也更长;婴幼儿,尤其是早产和低体质量儿更易发生低体温 BMI BMI<25 kg/m2是围术期低体温的独立危险因素;超重患者有矛盾结论:BMI越大,热量散失越快;但肥胖患者由于脂肪保护作用,体表散热减少,核心体温与体表温度差值减小;内脏型肥胖患者的腰臀比可作为腔镜手术低体温发生的危险因素之一 ASA分级 ASA Ⅱ级以上患者低体温发生率高于ASA Ⅰ级患者,且ASA分级越高,围术期低体温发生风险越高 基础体温 基础体温是影响围术期低体温的独立高风险因素,术前体温偏低患者围术期低体温发生风险明显增高 合并症 合并代谢性疾病可影响体温:如糖尿病合并神经病变患者围术期低体温发生风险增加 手术因素 手术分级 手术分级越高,患者围术期低体温发生率越高 手术类型 开放性手术体腔暴露,腔镜手术建立CO2气腹及术中大量冲洗液均易导致围术期低体温的发生 手术时间 手术时间超过2 h,围术期低体温发生率明显增高,全身麻醉患者尤甚 术中冲洗 使用超过1000 mL未加温冲洗液,患者围术期低体温发生率增高 术中输液/输血 静脉输注1000 mL室温晶体液或1个单位2~6 ℃库存血,可使体温下降0.25~0.5 ℃;静脉输注未加温液体超过1000 mL时,围术期低体温发生风险增高 麻醉因素 麻醉方式 全身麻醉较椎管内或区域麻醉围术期低体温发生率高;复合麻醉方式(如全身麻醉复合椎管内或区域麻醉)较单纯全身麻醉围术期低体温发生率高 麻醉平面 椎管内麻醉平面越高,核心体温越低 麻醉时间 麻醉时间超过2 h, 患者围术期低体温发生率增高 麻醉药物 吸入性麻醉药、静脉麻醉药及麻醉性镇痛药均可影响体温调节机制,导致围术期低体温发生 环境因素 手术室温度 增加环境温度对患者围术期低体温的发生具有保护作用,通常低于21 ℃患者低体温发生风险增高 BMI:体质量指数;ASA:美国麻醉医师协会  下载: 导出CSV
下载: 导出CSV
表 3 围术期体温监测
项目 具体描述 体温监测时长 理想状态下,体温监测应具连续性,涵盖术前、术中和术后 体温监测频率 术前 接患者前,应在病房测量1次;手术等候区可每15~30分钟测量1次 术中 记录入室和出室体温,推荐连续监测体温,可每15~30分钟测量1次,直至手术结束 术后 记录出入麻醉恢复室体温,连续监测体温,至少每15~30分钟测量1次 体温监测部位 核心体温 肺动脉、食管下段1/3、鼻咽部(鼻孔至鼻咽上部1/3)、鼓膜;在全身麻醉期间,食管或鼻咽通常是最实用的体温监测部位 近似核心体温 规范测量的口腔、腋窝温度可近似于核心体温,适用于椎管内麻醉、区域阻滞患者;相反,膀胱、直肠温度欠准确,并存在延迟效应
下载: 导出CSV
-
[1] Sessler DI. Mild perioperative hypothermia[J]. N Engl J Med, 1997, 336: 1730-1737. DOI: 10.1056/NEJM199706123362407
[2] Mendonça FT, Ferreira J, Guilardi V, et al. Prevalence of inadvertent perioperative hypothermia and associated factors: a cross-sectional study[J]. Ther Hypothermia Temp Manag, 2021, 11: 208-215. DOI: 10.1089/ther.2020.0038
[3] Akers JL, Dupnick AC, Hillman EL, et al. Inadvertent perioperative hypothermia risks and postoperative complications: a retrospective study[J]. AORN J, 2019, 109: 741-747. DOI: 10.1002/aorn.12696
[4] Brustia R, Monsel A, Skurzak S, et al. Guidelines for Perioperative Care for Liver Transplantation: Enhanced Recovery After Surgery (ERAS) Recommendations[J]. Transplantation, 2022, 106: 552-561. DOI: 10.1097/TP.0000000000003808
[5] 国家麻醉专业质量控制中心, 中华医学会麻醉学分会. 围手术期患者低体温防治专家共识(2017)[J]. 协和医学杂志, 2017, 8: 352-358. DOI: 10.3969/j.issn.1674-9081.2017.06.007 [6] 陈颖, 王莹, 张越伦, 等. 全麻患者围手术期低体温风险预测模型的前瞻性、多中心研究[J]. 中国医学科学院学报, 2022, 44: 1028-1032. https://www.cnki.com.cn/Article/CJFDTOTAL-ZYKX202206012.htm [7] 陈耀龙, 杨克虎, 王小钦, 等. 中国制订/修订临床诊疗指南的指导原则(2022版)[J]. 中华医学杂志, 2022, 102: 697-703. DOI: 10.3760/cma.j.cn112137-20211228-02911 [8] Collins S, Budds M, Raines C, et al. Risk factors for perioperative hypothermia: a literature review[J]. J Perianesth Nurs, 2019, 34: 338-346. DOI: 10.1016/j.jopan.2018.06.003
[9] Sari S, Aksoy SM, But A. The incidence of inadvertent perioperative hypothermia in patients undergoing general anesthesia and an examination of risk factors[J]. Int J Clin Pract, 2021, 75: e14103.
[10] Scott AV, Stonemetz JL, Wasey JO, et al. Compliance with surgical care improvement project for body temperature management (SCIP Inf-10) is associated with improved clinical outcomes[J]. Anesthesiology, 2015, 123: 116-125. DOI: 10.1097/ALN.0000000000000681
[11] Sessler DI. Perioperative thermoregulation and heat balance[J]. Lancet, 2016, 387: 2655-2664. DOI: 10.1016/S0140-6736(15)00981-2
[12] Lenhardt R. Body temperature regulation and anesthesia[J]. Handb Clin Neurol, 2018, 157: 635-644.
[13] Joris J, Ozaki M, Sessler DI, et al. Epidural anesthesia impairs both central and peripheral thermoregulatory control during general anesthesia[J]. Anesthesiology, 1994, 80: 268-277. DOI: 10.1097/00000542-199402000-00006
[14] Sessler DI. Perioperative temperature monitoring[J]. Anesthesiology, 2021, 134: 111-118. DOI: 10.1097/ALN.0000000000003481
[15] Frank SM, Fleisher LA, Breslow MJ, et al. Perioperative maintenance of normothermia reduces the incidence of morbid cardiac events. A randomized clinical trial[J]. JAMA, 1997, 277: 1127-1134. DOI: 10.1001/jama.1997.03540380041029
[16] Bindu B, Bindra A, Rath G. Temperature management under general anesthesia: Compulsion or option[J]. J Anaesthesiol Clin Pharmacol, 2017, 33: 306-316. DOI: 10.4103/joacp.JOACP_334_16
[17] Kurz A, Sessler DI, Lenhardt R. Perioperative normothermia to reduce the incidence of surgical-wound infection and shorten hospitalization. Study of Wound Infection and Temperature Group[J]. N Engl J Med, 1996, 334: 1209-1215. DOI: 10.1056/NEJM199605093341901
[18] Balki I, Khan JS, Staibano P, et al. Effect of perioperative active body surface warming systems on analgesic and clinical outcomes: a systematic review and meta-analysis of randomized controlled trials[J]. Anesth Analg, 2020, 131: 1430-1443. DOI: 10.1213/ANE.0000000000005145
[19] Sessler DI, Pei L, Li K, et al. Aggressive intraoperative warming versus routine thermal management during non-cardiac surgery (PROTECT): a multicentre, parallel group, superiority trial[J]. Lancet, 2022, 399: 1799-1808. DOI: 10.1016/S0140-6736(22)00560-8
[20] Pasquier M, Paal P, Kosinski S, et al. Esophageal temperature measurement[J]. N Engl J Med, 2020, 383: e93. DOI: 10.1056/NEJMvcm1900481
[21] Wang M, Singh A, Qureshi H, et al. Optimal depth for nasopharyngeal temperature probe positioning[J]. Anesth Analg, 2016, 122: 1434-1438. DOI: 10.1213/ANE.0000000000001213
[22] Pei L, Huang Y, Mao G, et al. Axillary Temperature, as Recorded by the iThermonitor WT701, Well Represents Core Temperature in Adults Having Noncardiac Surgery[J]. Anesth Analg, 2018, 126: 833-838. DOI: 10.1213/ANE.0000000000002706
[23] Thapa HP, Kerton AJ, Peyton PJ. Comparison of the EasyWarm® self-heating blanket with the Cocoon forced-air warming blanket in preventing intraoperative hypothermia[J]. Anaesth Intensive Care, 2019, 47: 169-174. DOI: 10.1177/0310057X19840264
[24] Min SH, Yoon S, Yoon SH, et al. Randomised trial comparing forced-air warming to the upper or lower body to prevent hypothermia during thoracoscopic surgery in the lateral decubitus position[J]. Br J Anaesth, 2018, 120: 555-562. DOI: 10.1016/j.bja.2017.11.091
[25] Cobb B, Cho Y, Hilton G, et al. Active warming utilizing combined Ⅳ fluid and forced-air warming decreases hypothermia and improves maternal comfort during cesarean delivery: a randomized control trial[J]. Anesth Analg, 2016, 122: 1490-1497. DOI: 10.1213/ANE.0000000000001181
[26] Thiel B, Mooijer BC, Kolff-Gart AS, et al. Is preoperative forced-air warming effective in the prevention of hypothermia in orthopedic surgical patients? A randomized controlled trial[J]. J Clin Anesth, 2020, 61: 109633. DOI: 10.1016/j.jclinane.2019.109633
[27] Lee Y, Kim K. Optimal application of forced air warming to prevent peri-operative hypothermia during abdominal surgery: a systematic review and meta-analysis[J]. Int J Environ Res Public Health, 2021, 18: 2517. DOI: 10.3390/ijerph18052517
[28] Roxby D, Sobieraj-Teague M, von Wielligh J, et al. Warming blood prior to transfusion using latent heat[J]. Emerg Med Australas, 2020, 32: 604-610. DOI: 10.1111/1742-6723.13471
[29] Wittenborn J, Mathei D, van Waesberghe J, et al. The effect of warm and humidified gas insufflation in gynecolo-gical laparoscopy on maintenance of body temperature: a prospective randomized controlled multi-arm trial[J]. Arch Gynecol Obstet, 2022, 306: 753-767. DOI: 10.1007/s00404-022-06499-z
[30] Shaw CA, Steelman VM, DeBerg J, et al. Effectiveness of active and passive warming for the prevention of inadvertent hypothermia in patients receiving neuraxial anesthesia: a systematic review and meta-analysis of randomized controlled trials[J]. J Clin Anesth, 2017, 38: 93-104. DOI: 10.1016/j.jclinane.2017.01.005
[31] Kim HY, Lee KC, Lee MJ, et al. Comparison of the efficacy of a forced-air warming system and circulating-water mattress on core temperature and post-anesthesia shivering in elderly patients undergoing total knee arthroplasty under spinal anesthesia[J]. Korean J Anesthesiol, 2014, 66: 352-357. DOI: 10.4097/kjae.2014.66.5.352
[32] Yasar PO, Uzumcugil F, Pamuk AG, et al. Comparison of combined forced-air warming and circulating-water-mattress and forced-air warming alone in patients undergoing open abdominal surgery in lithotomy position: a randomized controlled trial[J]. Indian J Surg, 2022, 84: 72-78. DOI: 10.1007/s12262-021-02829-8
[33] Soysal GE, Ilçe A, Erkol MH. Effect of "an innovative technology" active warming and passive warming on unplanned hypothermia during perioperative period: a clinical trial[J]. Ther Hypothermia Temp Manag, 2018, 8: 216-224. DOI: 10.1089/ther.2017.0048
[34] Cao J, Sheng X, Ding Y, et al. Effect of warm bladder irrigation fluid for benign prostatic hyperplasia patients on perioperative hypothermia, blood loss and shiver: a meta-analysis[J]. Asian J Urol, 2019, 6: 183-191. DOI: 10.1016/j.ajur.2018.07.001
[35] Oderda M, Cerutti E, Gontero P, et al. The impact of warmed and humidified CO(2) insufflation during robotic radical prostatectomy: results of a randomized controlled trial[J]. Urologia, 2019, 86: 130-140. DOI: 10.1177/0391560319834837
[36] Jiang R, Sun Y, Wang H, et al. Effect of different carbon dioxide (CO2) insufflation for laparoscopic colorectal surgery in elderly patients: a randomized controlled trial[J]. Medicine (Baltimore), 2019, 98: e17520. DOI: 10.1097/MD.0000000000017520
[37] Pei L, Huang Y, Xu Y, et al. Effects of ambient temperature and forced-air warming on intraoperative core temperature: a factorial randomized trial[J]. Anesthesiology, 2018, 128: 903-911. DOI: 10.1097/ALN.0000000000002099
[38] National Institute for Health and Care Excellence. Hypothermia: prevention and management in adults having surgery[EB/OL]. (2016-12-14)[2023-06-03]. https://www.nice.org.uk/guidance/CG65/chapter/Recommendations#intraoperative-phase.
[39] Duryea EL, Nelson DB, Wyckoff MH, et al. The impact of ambient operating room temperature on neonatal and maternal hypothermia and associated morbidities: a randomized controlled trial[J]. Am J Obstet Gynecol, 2016, 214: 505. e1-505. e7.
[40] Lai LL, See MH, Rampal S, et al. Significant factors influencing inadvertent hypothermia in pediatric anesthesia[J]. J Clin Monit Comput, 2019, 33: 1105-1112. DOI: 10.1007/s10877-019-00259-2
[41] Rauch S, Miller C, Bräuer A, et al. Perioperative hypothermia: a narrative review[J]. Int J Environ Res Public Health, 2021, 18: 8749. DOI: 10.3390/ijerph18168749
[42] Palanisamy S, Rudingwa P, Panneerselvam S, et al. Effect of low dose phenylephrine infusion on shivering and hypothermia in patients undergoing cesarean section under spinal anesthesia: a randomized clinical trial[J]. Int J Obstet Anesth, 2022, 50: 103542. DOI: 10.1016/j.ijoa.2022.103542
[43] Gupta N, Bharti SJ, Kumar V, et al. Comparative evaluation of forced air warming and infusion of amino acid-enriched solution on intraoperative hypothermia in patients undergoing head and neck cancer surgeries: a prospective randomised study[J]. Saudi J Anaesth, 2019, 13: 318-324. DOI: 10.4103/sja.SJA_839_18
[44] Mizobe T, Nakajima Y, Ueno H, et al. Fructose administration increases intraoperative core temperature by augmenting both metabolic rate and the vasoconstriction threshold[J]. Anesthesiology, 2006, 104: 1124-1130. DOI: 10.1097/00000542-200606000-00005
[45] Yi J, Zhan L, Lei Y, et al. Establishment and validation of a prediction equation to estimate risk of intraoperative hypothermia in patients receiving general anesthesia[J]. Sci Rep, 2017, 7: 13927. DOI: 10.1038/s41598-017-12997-x
[46] Dai Z, Zhang Y, Yi J, et al. Validation of a prediction model for intraoperative hypothermia in patients receiving general anesthesia[J]. Int J Clin Pract, 2022, 2022: 6806225.
[47] Yoo JH, Ok SY, Kim SH, et al. Efficacy of active forced air warming during induction of anesthesia to prevent inadvertent perioperative hypothermia in intraoperative warming patients: comparison with passive warming, a randomized controlled trial[J]. Medicine (Baltimore), 2021, 100: e25235. DOI: 10.1097/MD.0000000000025235
[48] Xiong Z, Zhu J, Li Q, et al. The effectiveness of warming approaches in preventing perioperative hypothermia: systematic review and meta-analysis[J]. Int J Nurs Pract, 2022. doi: 10.1111/ijn.13100.
[49] Van Duren A. Perioperative prewarming: heat transfer and physiology[J]. AORN J, 2022, 115: 407-422. DOI: 10.1002/aorn.13667
[50] Connelly L, Cramer E, DeMott Q, et al. The optimal time and method for surgical prewarming: a comprehen-sive review of the literature[J]. J Perianesth Nurs, 2017, 32: 199-209. DOI: 10.1016/j.jopan.2015.11.010
[51] Ni TT, Zhou ZF, He B, et al. Effects of combined warmed preoperative forced-air and warmed perioperative intravenous fluids on maternal temperature during cesarean section: a prospective, randomized, controlled clinical trial[J]. BMC Anesthesiol, 2020, 20: 48. DOI: 10.1186/s12871-020-00970-7
[52] Liu J, Wang Y, Ma W. Shivering prevention and treatment during cesarean delivery under neuraxial anesthesia: a systematic review[J]. Minerva Anestesiol, 2018, 84: 1393-1405.
[53] Zhuo Q, Xu JB, Zhang J, et al. Effect of active and passive warming on preventing hypothermia and shivering during cesarean delivery: a systematic review and meta-analysis of randomized controlled trials[J]. BMC Pregnancy Childbirth, 2022, 22: 720. DOI: 10.1186/s12884-022-05054-7
[54] Dendis M, Hooven K. Preventing hypothermia during cesarean birth: an integrative review[J]. MCN Am J Matern Child Nurs, 2020, 45: 102-108. DOI: 10.1097/NMC.0000000000000599
[55] Sun Y, Jia LL, Yu WL, et al. The changes of intraoperative body temperature in adult liver transplantation: A retrospective study[J]. Hepatobiliary Pancreat Dis Int, 2018, 17: 496-501. DOI: 10.1016/j.hbpd.2018.08.006
[56] Perlman R, Callum J, Laflamme C, et al. A recommended early goal-directed management guideline for the prevention of hypothermia-related transfusion, morbidity, and mortality in severely injured trauma patients[J]. Crit Care, 2016, 20: 107. DOI: 10.1186/s13054-016-1271-z
-
期刊类型引用(3)
1. 祝健婵,熊小琴,刘海燕. 加速康复外科理念及电生理技术对妇科腹腔镜术后患者肠道功能恢复的研究. 实用妇科内分泌电子杂志. 2024(19): 80-82+119 .  百度学术
百度学术
2. 李金科,欧阳玲. 加速康复外科理念在卵巢癌围手术期应用的研究进展. 现代肿瘤医学. 2023(18): 3507-3511 . 百度学术
3. 李哲. 中西医结合护理在宫颈癌患者围手术期中临床应用价值评价. 辽宁中医药大学学报. 2020(08): 197-199 . 百度学术
其他类型引用(2)
计量
- 文章访问数: 4409
- HTML全文浏览量: 587
- PDF下载量: 2782
- 被引次数: 5












