 作者投稿
作者投稿 专家审稿
专家审稿 编辑办公
编辑办公 邮件订阅
邮件订阅 RSS
RSS

Relationship between Non-sustained Ventricular Tachycardia before Implantation and Appropriate Therapy in Patients with Implantable Cardioverter Defibrillator for Primary Prevention of Sudden Cardiac Death
-
摘要:
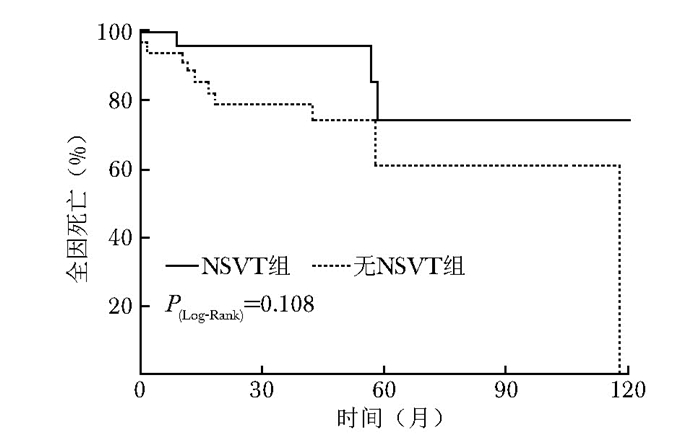
目的 探讨植入型心律转复除颤器(implantable cardioverter defibrillator, ICD)用于心源性猝死一级预防时, 植入前发生非持续性室性心动过速(non-sustained ventricular tachycardia, NSVT)与植入后ICD恰当治疗的关系。 方法 本研究为单中心回顾性队列研究, 连续纳入2006年1月至2017年12月在北京协和医院住院植入ICD用于一级预防的心脏病患者, 患者在住院期间ICD植入前均完善Holter检查。根据Holter检查是否出现NSVT, 将患者分为NSVT组及无NSVT组。门诊或电话随访至2018年8月, 随访事件包括全因死亡、植入后ICD放电治疗及抗心动过速起搏(antitachycardia pacing, ATP)治疗情况。 结果 纳入60例符合入选和排除标准的患者, 随访时间37(14~61)个月, Kaplan-Meier生存曲线及Log-Rank检验提示, NSVT组与无NSVT组相比, 全因死亡率无统计学差异(P=0.108), NSVT组恰当治疗的风险高于无NSVT组(P=0.033), NSVT和左心室射血分数与ICD恰当治疗独立相关(NSVT:HR=5.099, 95% CI:1.399~18.588, P=0.014;左心室射血分数:HR=1.077, 95% CI:1.013~1.145, P=0.018)。 结论 ICD一级预防患者植入前出现NSVT提示接受ICD恰当治疗的风险增加。 -
关键词:
- 植入型心律转复除颤器 /
- 非持续性室性心动过速 /
- 恰当治疗 /
- 全因死亡 /
- 左心室射血分数
Abstract:Objective The aim of this study was to explore the relationship between non-sustained ventricular tachycardia (NSVT) recorded by Holter before implantation and appropriate therapy in patients with implantable cardioverter defibrillator (ICD) for primary prevention of sudden cardiac death. Methods A single-center retrospective cohort study was conducted. Consecutive inpatients who received ICD for primary prevention and finished Holter examination from January 2006 to December 2017 in Peking Union Medical College Hospital were enrolled. According to the results of Holter, the patients were divided into the NSVT group and the non-NSVT group. Clinic or telephone follow-ups were conducted until August 2018; the follow-up events included all-cause death, shock therapy, and anti-tachycardia pacing (ATP). Results Sixty patients meeting the inclusive and exclusive criteria were enrolled in this study. Median follow-up of all patients was 37 (14-61) months. Kaplan-Meier curve and Log-Rank test showed that there was no significant difference in mortality between the NSVT and the non-NSVT group (P=0.108), while the NSVT group had a significantly higher rate of appropriate therapy (P=0.033). Multivariate competitive risk regression analysis indicated that NSVT and left ventricular ejection fraction were independently correlated with the ICD appropriate therapy (NSVT: HR=5.099, 95% CI:1.399-18.588, P=0.014; left ventricular ejection fraction: HR=1.077, 95% CI:1.013-1.145, P=0.018). Conclusion NSVT in patients with ICD implantation for primary prevention suggests an increased risk of receiving appropriate therapy. 利益冲突 无 -
表 1 两组植入心律转复除颤器一级预防患者一般临床资料比较
临床指标 总体(n=60) 无NSVT组(n=36) NSVT组(n=24) P值 男性[n(%)] 44(73.3) 26(72.2) 18(75.0) 0.812 年龄[M(QR),岁] 63(50, 71) 65(50, 73) 60.5(50, 68) 0.274 NYHA分级≥Ⅲ [n(%)] 30(50.0) 17(47.2) 13(54.2) 0.598 收缩压(x±s, mmHg) 117.05±17.48 120.64±18.16 111.67±15.21 0.051 舒张压(x±s, mmHg) 71.95±12.34 74.61±11.60 67.96±12.62 0.040 心率[M(QR,次/min] 75(60, 84) 72(60, 80) 77(61, 87) 0.398 QRSD[M(QR,ms] 120(104, 149) 119.5(97, 157) 121(109, 135) 0.746 植入CRTD[n(%)] 14(23.3) 9(25.0) 5(20.8) 0.709 左心房前后径[M(QR),mm] 45(41, 52) 44(40, 50) 48(42, 53) 0.107 左心室收缩末内径(x±s, mm) 54.12±10.47 52.89±10.95 55.96±9.64 0.270 LVEF[M(QR),%] 30(25, 35) 30(25, 35) 31(23, 37.5) 0.958 血肌酐[M(QR),μmol/L] 88(77, 98) 85(77, 95) 91(77, 101) 0.390 既往病史[n(%)] 缺血性心脏病 33(55.0) 21(58.3) 12(50.0) 0.525 心肌梗死 28(46.7) 20(55.6) 8(33.3) 0.091 高血压 30(50.0) 16(44.4) 14(58.3) 0.292 糖尿病 13(21.7) 9(25.0) 4(16.7) 0.443 房颤 16(26.7) 10(27.8) 6(15.0) 0.812 NSVT:非持续性室性心动过速; NYHA:纽约心脏协会; QRSD:QRS间期; CRTD:心脏再同步化除颤器; LVEF:左心室射血分数  下载: 导出CSV
下载: 导出CSV
表 2 两组植入心律转复除颤器一级预防患者随访事件比较
随访事件 总体(n=60) 无NSVT组(n=36) NSVT组(n=24) P值 随访时间[M(QR),月] 37(14~61) 40(14~62) 27(14~61) 0.964 恰当治疗事件[n(%)] 12(20.0) 4(11.1) 8(33.3) 0.035 首次恰当治疗时间[M(QR),月] 12(1~34) 18(4~44) 9(1~34) 0.732 全因死亡[n(%)] 14(23.3) 11(30.6) 3(12.5) 0.105 NSVT:同表 1
下载: 导出CSV
表 3 单因素竞争风险回归分析ICD恰当治疗危险因素
危险因素 HR 95% CI P值 男性 1.155 0.318~4.200 0.827 年龄 0.985 0.947~1.024 0.441 植入前NSVT 3.847 1.174~12.60 0.026 NYHA分级≥3 0.384 0.122~1.205 0.101 收缩压 1.007 0.970~1.046 0.710 舒张压 0.982 0.937~1.029 0.446 QRSD 0.999 0.845~1.012 0.845 CRTD 0.265 0.037~1.914 0.188 左心房前后径 0.946 0.859~1.041 0.256 左心室收缩末内径 0.947 0.895~1.002 0.058 LVEF 1.056 1.000~1.115 0.048 血肌酐 1.017 0.975~1.062 0.431 缺血性心脏病 1.521 0.456~5.066 0.495 心肌梗死 0.725 0.236~2.227 0.574 高血压 1.394 0.449~4.333 0.566 糖尿病 0.606 0.136~2.698 0.511 房颤 0.199 0.028~1.407 0.106 NSVT、NYHA、QRSD、CRTD、LVEF:同表 1
下载: 导出CSV
-
[1] Kostis JB, McCrone K, Moreyra AE, et al. Premature ventricular complexes in the absence of identifiable heart disease[J]. Circulation, 1981, 63:1351-1356. doi: 10.1161/01.CIR.63.6.1351 [2] Camm AJ, Evans KE, Ward DE, et al. The rhythm of the heart in active elderly subjects[J]. Am Heart J, 1980, 99:598-603. doi: 10.1016/0002-8703(80)90733-4 [3] Meinertz T, Hofmann T, Kasper W, et al. Significance of ventricular arrhythmias in idiopathic dilated cardiomyopathy[J]. Am J Cardiol, 1984, 53:902-907. doi: 10.1016/0002-9149(84)90522-8 [4] Massing MW, Simpson RJ, Rautaharju PM, et al. Usefulness of ventricular premature complexes to predict coronary heart disease events and mortality (from the Atherosclerosis Risk In Communities cohort)[J]. Am J Cardiol, 2006, 98:1609-1612. doi: 10.1016/j.amjcard.2006.06.061 [5] Agarwal SK, Heiss G, Rautaharju PM, et al. Premature ventricular complexes and the risk of incident stroke:the Atherosclerosis Risk In Communities (ARIC) Study[J]. Stroke, 2010, 41:588-593. doi: 10.1161/STROKEAHA.109.567800 [6] Cheriyath P, He F, Peters I, et al. Relation of atrial and/or ventricular premature complexes on a two-minute rhythm strip to the risk of sudden cardiac death (the Atherosclerosis Risk in Communities[ARIC] study)[J]. Am J Cardiol, 2011, 107:151-155. doi: 10.1016/j.amjcard.2010.09.002 [7] Lee V, Hemingway H, Harb R, et al. The prognostic significance of premature ventricular complexes in adults without clinically apparent heart disease:a meta-analysis and systematic review[J]. Heart, 2012, 98:1290-1298. doi: 10.1136/heartjnl-2012-302005 [8] Bergau L, Willems R, Sprenkeler DJ, et al. Differential multivariable risk prediction of appropriate shock versus competing mortality-A prospective cohort study to estimate benefits from ICD therapy[J]. Int J Cardiol, 2018, 272:102-107. doi: 10.1016/j.ijcard.2018.06.103 [9] Killu AM, Mazo A, Grupper A, et al. Super-response to cardiac resynchronization therapy reduces appropriate implantable cardioverter defibrillator therapy[J]. Europace, 2018, 20:1303-1311. doi: 10.1093/europace/eux235 [10] Teerlink JR, Jalaluddin M, Anderson S, et al. Ambulatory ventricular arrhythmias in patients with heart failure do not specifically predict an increased risk of sudden death. PROMISE (Prospective Randomized Milrinone Survival Evaluation) Investigators[J]. Circulation, 2000, 101:40-46. doi: 10.1161/01.CIR.101.1.40 [11] Yokoshiki H, Shimizu A, Mitsuhashi T, et al. Prognostic significance of nonsustained ventricular tachycardia in patients receiving cardiac resynchronization therapy for primary preven-tion:Analysis of the Japan cardiac device treatment registry database[J]. J Arrhythm, 2018, 34:139-147. doi: 10.1002/joa3.12023 [12] Chen J, Johnson G, Hellkamp AS, et al. Rapid-rate nonsustained ventricular tachycardia found on implantable cardioverter-defibrillator interrogation:relationship to outcomes in the SCD-HeFT (Sudden Cardiac Death in Heart Failure Trial)[J]. J Am Coll Cardiol, 2013, 61:2161-2168. doi: 10.1016/j.jacc.2013.02.046 [13] Jiménez-Candil J, Hernández J, Perdiguero P, et al. Prognostic significance of nonsustained ventricular tachycardia episodes occurring early after implantable cardioverter-defibrillator implantation among patients with left ventricular dysfunction[J]. Am J Cardiol, 2016, 118:1503-1510. doi: 10.1016/j.amjcard.2016.08.015 [14] Lee DS, Hardy J, Yee R, et al. Clinical risk stratification for primary prevention implantable cardioverter defibrillators[J]. Circ Heart Fail, 2015, 8:927-937. doi: 10.1161/CIRCHEARTFAILURE.115.002414 [15] Zhou Y, Zhao S, Chen K, et al. Predictive value of rapid-rate non-sustained ventricular tachycardia in the occurrence of appropriate implantable cardioverter-defibrillator therapy[J]. J Interv Card Electrophysiol, 2019.doi: 10.1007/s10840-019-00557-4.[Epub ahead of print]. [16] Koller MT, Schaer B, Wolbers M, et al. Death without prior appropriate implantable cardioverter-defibrillator therapy:a competing risk study[J]. Circulation, 2008, 117:1918-1926. doi: 10.1161/CIRCULATIONAHA.107.742155 [17] Sticherling C, Arendacka B, Svendsen JH, et al. Sex differences in outcomes of primary prevention implantable cardioverter-defibrillator therapy:combined registry data from eleven European countries[J]. Europace, 2018, 20:963-970. doi: 10.1093/europace/eux176 [18] Seegers J, Conen D, Jung K, et al. Sex difference in appropriate shocks but not mortality during long-term follow-up in patients with implantable cardioverter-defibrillators[J]. Europace, 2016, 18:1194-1202. doi: 10.1093/europace/euv361 [19] van der Heijden AC, Thijssen J, Borleffs CJ, et al. Gender-specific differences in clinical outcome of primary prevention implantable cardioverter defibrillator recipients[J]. Heart, 2013, 99:1244-1249. doi: 10.1136/heartjnl-2013-304013 [20] van Rees JB, Borleffs CJ, van Welsenes GH, et al. Clinical prediction model for death prior to appropriate therapy in primary prevention implantable cardioverter defibrillator patients with ischaemic heart disease:the FADES risk score[J]. Heart, 2012, 98:872-877. doi: 10.1136/heartjnl-2011-300632 -

 点击查看大图
点击查看大图

图(2) / 表(3)
计量
- 文章访问数: 441
- HTML全文浏览量: 29
- PDF下载量: 94
- 被引次数: 0












