 作者投稿
作者投稿 专家审稿
专家审稿 编辑办公
编辑办公 邮件订阅
邮件订阅 RSS
RSS

-
摘要:
目的 探讨经会阴模板引导前列腺饱和穿刺活检(transperineal template-guided prostate saturation biopsy,TTPSB)的安全性和可行性。 方法 回顾性分析苏北人民医院泌尿外科2017年3月至2018年5月收治的疑似前列腺癌行前列腺穿刺活检患者的临床资料。根据前列腺形态及大小、耻骨条件、患者意愿,将患者分为两组,一组行TTPSB,另一组行传统经会阴模板引导前列腺穿刺(transperineal template-guided prostate biopsy,TTPB)。比较两组穿刺术后并发症(出血、感染、尿潴留、排尿功能及勃起功能等)的发生情况。 结果 共纳入385例符合入选和排除标准的患者,TTPSB组204例,穿刺针数11~47针,平均(23.7±5.8)针;TTPB组181例,穿刺针数5~12针,平均(12.3±4.3)针;两组基线资料匹配。TTPSB组除中度血尿发生率较TTPB组高外[19.6% (40/216)比11.6% (21/181),P < 0.05],其余并发症发生率两组间均无统计学差异(P均 > 0.05)。两组国际前列腺症状评分(International Prostate Symptom Score,IPSS)穿刺后1、4周较穿刺前均升高[TTPSB组:15.8±6.9和12.6±7.5比10.2±6.8;TTPB组:16.2±6.7和13.2±7.1比10.7±7.2,P均 < 0.05],穿刺后12周两组IPSS恢复至穿刺前水平(TTPSB组:11.3±6.5;TTPB组:11.9± 6.8,P均 > 0.05)。比较两组国际勃起功能指数(International Index Erectile Function,IIEF)-5评分,穿刺后1个月均较穿刺前下降(TTPSB组:18.4±4.3比19.5±4.6;TTPB组:18.8±4.8比19.9±4.5,P均 < 0.05),而穿刺后3、6个月两组患者的IIEF-5评分(TTPSB组:18.9±4.4, 19.3±4.2;TTPB组:19.3±4.2, 19.7±4.3)与穿刺前相比均无统计学差异(P均 > 0.05)。 结论 与传统TTPB相比,TTPSB并发症不显著增加,是一种较安全的穿刺方法。 Abstract:Objective The aim of this study was to investigate the safety and feasibility of transperineal template-guided prostate biopsy (TTPSB). Methods Clinical data of patients with suspected prostate cancer who were admitted for prostate biopsy in the Department of Urology at the Northern Jiangsu People's Hospital from March 2017 to May 2018 were retrospectively collected and analyzed. All patients were divided into two groups, TTPSB group and traditional transperineal template-guided prostate biopsy (TTPB) group, according to the prostate shape and size, pubic condition, and patient intention. The complications including bleeding, infection, urinary retention, urinary function, and erectile function after prostate biopsy were compared between the two groups. Results A total of 385 patients meeting the inclusive and exclusive criteria were enrolled in this study. There were 204 patients in the TTPSB group with mean of (23.7±5.8) cores (range from 11 to 47 cores) and 181 patients in the TTPB group with mean of (12.3±4.3) cores (range from 5 to 12 cores); the baseline information was matched between the two groups. The incidence of moderate hematuria in the TTPSB group was higher than that in the TTPB group [19.6% (40/216) vs. 11.6% (21/181), P < 0.05]; there was no statistical difference in the incidence of the other complications (all P > 0.05). The International Prostate Symptom Score (IPSS) of the two groups were increased at the 1st and 4th week after the biopsy compared with the baseline before the biopsy [TTPSB group: 15.8±6.9 and 12.6±7.5 vs. 10.2±6.8; TTPB group: 16.2±6.7 and 13.2±7.1 vs. 10.7±7.2, all P < 0.05], and returned to the baseline level at the 12th week after the biopsy (TTPSB group: 11.3±6.5; TTPB group: 11.9±6.8, both P > 0.05). The International Index Erectile Function (IIEF-5) score of the two groups were decreased at the 1st month after biopsy compared with the baseline [TTPSB group: 18.4±4.3 vs. 19.5±4.6; TTPB group: 18.8±4.8 vs. 19.9±4.5, both P < 0.05]; while there was no significant difference between the baseline and the 3rd and 6th month after the biopsy (TTPSB group: 18.9± 4.4 and 19.3±4.2; TTPB group: 19.3±4.2 and 19.7±4.3, all P < 0.05). Conclusions Compared with traditonal TTPB, the complications of TTPSB are nearly the same. TTPSB is a safe procedure. -
Key words:
- prostate cancer /
- saturation biopsy /
- complication
利益冲突 无 -

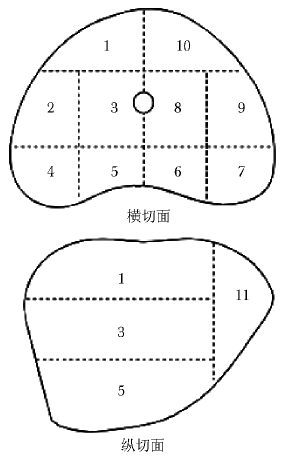
图 1 前列腺横纵切面各区分布示意图
1区:右前区;2区:右中外区;3区:右中区;4区:右后外侧角;5区:右后区;6区:左后区;7区:左后外侧角;8区:左中区;9区:左中外区;10区:左前区;11区:前列腺尖部
表 1 TTPSB和TTPB两组患者一般临床资料比较
分组 年龄(x±s,岁) PSA(x±s,ng/ml) 穿刺针数(x±s,针) 前列腺体积(x±s,ml) 使用抗凝药物的患者[n(%)] TTPSB组(n=204) 68.4±5.9 15.4±3.6 23.7±5.8 47.1±23.6 12(5.9) TTPB组(n=181) 67.5±6.7 14.8±3.8 12.3±4.3 45.8±25.7 10(5.5) t/χ2值 1.41 1.59 21.68 0.52 0.023 P值 0.16 0.11 <0.01 0.61 0.88 TTPSB:经会阴模板引导前列腺饱和穿刺活检;TTPB:经会阴模板引导前列腺穿刺活检; PSA:前列腺特异抗原  下载: 导出CSV
下载: 导出CSV
表 2 TTPSB和TTPB两组患者穿刺后并发症比较[n(%)]
并发症 TTPSB组(n=204) TTPB组(n=181) χ2值 P值 血尿 70(34.3) 56(30.9) 0.496 0.481 轻度 28(13.9) 34(18.7) 1.643 0.200 中度 40(19.6) 21(11.6) 4.610 0.032 重度 2( 1.0) 1( 0.6) 0.227 0.634 感染 2( 1.0) 2( 1.1) 0.014 0.904 尿潴留 4( 2.0) 3( 1.7) 0.049 0.824 会阴部血肿 15( 7.4) 10( 5.5) 0.528 0.468 轻度 8( 3.9) 5( 2.8) 0.395 0.530 中度 5( 2.5) 4( 2.2) 0.024 0.876 重度 2( 1.0) 1( 0.6) 0.227 0.634 血精 6( 2.9) 5( 2.8) 0.011 0.916 血便 0(0) 0(0) - - TTPSB、TTPB:同表 1
下载: 导出CSV
-
[1] Chen W, Zheng R, Baade PD, et al. Cancer statistics in China, 2015 [J]. CA Cancer J Clin, 2016, 66: 115-132. doi: 10.3322/caac.21338 [2] Ploussard G, Nicolaiew N, Marchand C, et al. Prospective evaluation of an extended 21-core biopsy scheme as initial prostate cancer diagnostic strategy [J]. Eur Urol, 2014, 65: 154-161. doi: 10.1016/j.eururo.2012.05.049 [3] 那彦群, 叶章群, 孙颖浩, 等.中国泌尿外科疾病诊断治疗指南[M].北京: 人民卫生出版社, 2014: 62-64. [4] 丁雪飞, 张立国, 周广臣, 等.模板定位下经会阴前列腺穿刺活检在经直肠途径初次活检阴性患者检查中的应用[J].中华泌尿外科杂志, 2013, 34: 298-300. doi: 10.3760/cma.j.issn.1000-6702.2013.04.019 [5] Radtke JP, Kuru TH, Boxler S, et al. Comparative analysis of transperineal template saturation prostate biopsy versus magnetic resonance imaging targeted biopsy with magnetic resonance imaging-ultrasound fusion guidance [J]. J Urol, 2015, 193: 87-94. doi: 10.1016/j.juro.2014.07.098 [6] Loeb S, Vellekoop A, Ahmed HU, et al. Systematic review of complications of prostate biopsy [J]. Eur Urol, 2013, 64: 876-892. doi: 10.1016/j.eururo.2013.05.049 [7] Li H, Yan W, Zhou Y, et al. Transperineal ultrasound-guided saturation biopsies using 11-region template of prostate: report of 303 cases [J]. Urology, 2007, 70: 1157-1161. doi: 10.1016/j.urology.2007.07.072 [8] Yan W, Li H, Zhou Y, et al. Prostate carcinoma spatial distribution patterns in Chinese men investigated with systematic transperineal ultrasound guided 11-region biopsy [J]. Urol Oncol, 2009, 27: 520-524. doi: 10.1016/j.urolonc.2008.05.002 [9] Skouteris VM, Crawford ED, Mouraviev V, et al. Trans- rectal ultrasound-guided versus transperineal mapping prostate biopsy: complication comparison [J]. Rev Urol, 2018, 20: 19-25. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4630643/ [10] 严维刚, 李汉忠, 纪志刚, 等.经会阴模板定位前列腺11区饱和穿刺活检:附2066例分析[J].协和医学杂志, 2012, 3: 190-194. doi: 10.3969/j.issn.1674-9081.2012.02.013 [11] Borboroglu PG, Comer SW, Riffenburgh RH, et al. Extensive repeat transrectal ultrasound guided prostate biopsy in patients with previous benign sextant biopsies [J]. J Urol, 2000, 163: 158-162. doi: 10.1016/S0022-5347(05)67994-3 [12] Raaijmakers R, Kirkels WJ, Roobol MJ, et al. Complication rates and risk factors of 5802 transrectal ultrasound-guided sextant biopsies of the prostate within a population-based screening program [J]. Urology, 2002, 60: 826-830. doi: 10.1016/S0090-4295(02)01958-1 [13] Klein T, Palisaar RJ, Holz A, et al. The impact of prostate biopsy and periprostatic nerve block on erectile and voiding function: a prospective study [J]. J Urol, 2010, 184: 1447-1452. doi: 10.1016/j.juro.2010.06.021 [14] Akbal C, Türker P, Tavuku HH, et al. Erectile function in prostate cancer-free patients who underwent prostate saturation biopsy [J]. Eur Urol, 2008, 53: 540-544. doi: 10.1016/j.eururo.2007.06.039 [15] Badalyan R. Editorial comment on: erectile function in prostate cancer-free patients who underwent prostate saturation biopsy [J]. Eur Urol, 2008, 53: 545-546. doi: 10.1016/j.eururo.2007.06.041 [16] Pepe P, Pennisi M. Erectile dysfunction in 1050 men following extended (18 cores) vs saturation (28 cores) vs saturation plus MRI-targeted prostate biopsy (32 cores) [J]. Int J Impot Res, 2016, 28: 1-3. doi: 10.1038/ijir.2015.18 -

 点击查看大图
点击查看大图
图(1) / 表(4)
计量
- 文章访问数: 376
- HTML全文浏览量: 41
- PDF下载量: 47
- 被引次数: 0












