 作者投稿
作者投稿 专家审稿
专家审稿 编辑办公
编辑办公 邮件订阅
邮件订阅 RSS
RSS

Clinical Characteristics of Gleason Score 10 Prostate Cancer on Core Biopsy without Distant Metastases at Initial Diagnosis
-
摘要:
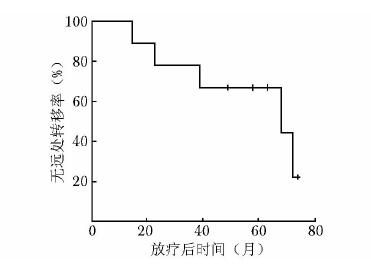
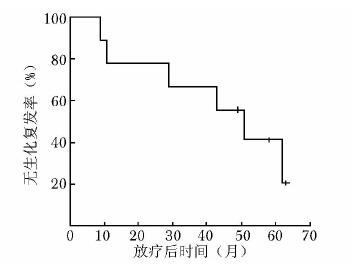
目的 分析初诊无远处转移的穿刺病理Gleason评分为10分前列腺癌的临床特点并探讨外放疗联合内分泌治疗的疗效。 方法 2003年1月至2014年3月北京协和医院收治初诊无远处转移的Gleason评分10分前列腺癌患者9例。所有患者均接受全盆腔外放疗联合长期内分泌治疗。全盆腔外放疗的照射剂量为50.0 Gy, 前列腺、双侧精囊腺及区域阳性淋巴结加量至76.2~78.0 Gy。内分泌治疗采用最大限度雄激素阻断:口服抗雄激素药物加每月注射一次黄体生成素释放激素类似物。分析患者临床特点及联合治疗效果, 并运用Kaplan-Meier法绘制生存曲线。 结果 患者中位随访时间为4.8年(26~75个月)。治疗前中位血清前列腺特异性抗原(prostate specific antigen, PSA)为11.2 μg/L, 其中6例低于20 μg/L, 3例高于70 μg/L。中位穿刺活检针数阳性率为90.9%。TNM分期:3例T2c, 4例T3a, 2例T3b; 6例N0, 3例N1; 9例M0。随访期间, 6例患者出现生化复发, 其中5例进一步发展为转移性前列腺癌; 4例患者死亡, 其中3例死于前列腺癌。5年无生化复发率、无远处转移率、肿瘤特异性生存率及总体生存率分别为28.6%、57.1%、66.7%和57.1%。5例出现1~2级早期放疗胃肠道不良反应, 6例出现1~2级早期泌尿系统不良反应, 无晚期胃肠道及泌尿系统不良反应。无骨折、心血管意外等严重内分泌治疗并发症。 结论 初诊无远处转移的穿刺病理Gleason评分10分前列腺癌常伴穿刺阳性范围大、肿瘤分期偏晚等高危因素, 患者通常预后不良, 放疗联合内分泌治疗等及时和积极的综合治疗方案往往是必需的。 Abstract:Objective To analyze the clinical characteristics of patients with Gleason score 10 prostate cancer on core biopsy and without distant metastases when first diagnosed, and to evaluate the effectiveness of external radiotherapy combined with hormone therapy in these patients. Methods From January 2003 to March 2014, 9 patients were identified as Gleason score 10 prostate cancer without distant metastases when first diagnosed at Peking Union Medical College Hospital. All the patients were treated by whole pelvic external radiotherapy and long-term hormone therapy. The whole pelvic radiation dose was 50.0 Gy, the boost dose for the whole prostate, bilateral seminal vesicles, and regional positive lymph nodes ranged from 76.2 to 78.0 Gy. The hormone therapy used maximal androgen blockade, i.e. oral anti-androgen drugs plus monthly injection of luteinizing hormone-releasing hormone analogs. We assessed the clinical characteristics of the patients and the treatment outcomes of the combination therapy. Survival curves were calculated using the Kaplan-Meier method. Results The median follow-up was 4.8 years (26-75 months). The median pre-treatment serum prostate specific antigen (PSA) level was 11.2 μg/L. The pre-treatment PSA levels were lower than 20 μg/L in 6 patients, and higher than 70 μg/L in 3 patients. The median percentage of positive biopsy cores was 90.9%. In TNM staging, 3, 4, and 2 cases were classified as T2c, T3a, and T3b, respectively; 6 and 3 cases were classified as N0 and N1, respectively; and all the 9 cases were classified as M0. Six patients developed biochemical failure, 5 of which progressed into distant metastasis. Four patients died during the follow-up period, 3 of which died of prostate cancer. The 5-year biochemical failure-free survival (BFFS), distant metastasis-free survival (DMFS), cancer-specific survival (CSS), and overall survival (OS) were 28.6%, 57.1%, 66.7%, and 57.1%, respectively. Five patients experienced grade 1-2 acute gastrointestinal (GI) toxicity and 6 patients developed grade 1-2 acute genitourinary (GU) toxicity due to radiotherapy. No late GI or GU toxicity was reported. No bone fracture, cardiovascular event, or other severe hormone therapy-related complications was detected. Conclusions Gleason score 10 prostate cancer without distant metastases when first diagnosed may be often combined with high risk factors such as high percentage of positive biopsy cores, and advanced tumor stage. Timely and active comprehensive treatments including external radiotherapy and hormone therapy are usually necessary because these patients generally have unfavorable prognosis. -
Key words:
- prostate cancer /
- biopsy pathology /
- combined therapy /
- treatment effect
-
[1] 那彦群, 叶章群, 孙颖浩, 等.中国泌尿外科疾病诊断治疗指南[M].北京:人民卫生出版社, 2014:65. [2] Hu XH, Cammann H, Meyer HA, et al. Risk prediction models for biochemical recurrence after radical prostatectomy using prostate-specific antigen and Gleason score[J]. Asian J Androl, 2014, 16:897-901. doi: 10.4103/1008-682X.129940 [3] McGuire BB, Helfand BT, Loeb S, et al. Outcomes in patients with Gleason score 8-10 prostate cancer:relation to preoperative PSA level[J]. BJU Int, 2012, 109:1764-1769. doi: 10.1111/j.1464-410X.2011.10628.x [4] Krauss DJ, Hayek S, Amin M, et al. Prognostic significance of neuroendocrine differentiation in patients with Gleason score 8-10 prostate cancer treated with primary radiotherapy[J]. Int J Radiat Oncol Biol Phys, 2011, 81:119-125. https://www.ncbi.nlm.nih.gov/pubmed/21596486 [5] Stock RG, Cesaretti JA, Hall SJ, et al. Outcomes for patients with high-grade prostate cancer treated with a combination of brachytherapy, external beam radiotherapy and hormonal therapy[J]. BJU Int, 2009, 104:1631-1636. doi: 10.1111/j.1464-410X.2009.08661.x [6] Ellis CL, Partin AW, Han M, et al. Adenocarcinoma of the prostate with Gleason score 9-10 on core biopsy:correlation with findings at radical prostatectomy and prognosis[J]. J Urol, 2013, 190:2068-2073. doi: 10.1016/j.juro.2013.05.056 [7] Humphrey PA. Gleason pattern 5 adenocarcinoma in prostate needle biopsy[J]. J Urol, 2012, 188:1341-1342. doi: 10.1016/j.juro.2012.06.126 [8] Sabolch A, Feng F, Daignault-Newton S, et al. Gleason pattern 5 is the greatest risk factor for clinical failure and death from prostate cancer after dose-escalated radiation therapy and hormonal ablation[J]. Int J Radiat Oncol Biol Phys, 2011, 81:351-360. http://www.ncbi.nlm.nih.gov/pubmed/21493015 [9] Nanda A, Chen M, Renshaw A, et al. Gleason pattern 5 prostate cancer:further stratification of patients with high-risk disease and implications for future randomized trials[J]. Int J Radiat Oncol Biol Phys, 2008, 74:1419-1423. https://www.ncbi.nlm.nih.gov/pubmed/19131185 [10] Yamamoto S, Masuda H, Urakami S, et al. Patient-perceived satisfaction after definitive treatment for men with high-risk prostate cancer:radical prostatectomy vs. intensity-modulated radiotherapy with androgen deprivation therapy[J]. Urology, 2015, 85:407-413. doi: 10.1016/j.urology.2014.09.046 [11] Roach M 3rd. Current trends for the use of androgen deprivation therapy in conjunction with radiotherapy for patients with unfavorable intermediate-risk, high-risk, localized, and locally advanced prostate cancer[J]. Cancer, 2014, 120:1620-1629. doi: 10.1002/cncr.28594 [12] Zelefsky MJ, Pei X, Chou JF, et al. Dose escalation for prostate cancer radiotherapy:predictors of long-term biochemical tumor control and distant metastases-free survival outcomes[J]. Eur Urol, 2011, 60:1133-1139. doi: 10.1016/j.eururo.2011.08.029 [13] Bolla M, de Reijke TM, Van Tienhoven G, et al. Duration of androgen suppression in the treatment of prostate cancer[J]. N Engl J Med, 2009, 360:2516-2527. doi: 10.1056/NEJMoa0810095 [14] Weir EG, Partin AW, Epstein JI. Correlation of serum prostate specific antigen and quantitative immunohistochemistry[J]. J Urol, 2000, 163:1739-1742. doi: 10.1016/S0022-5347(05)67532-5 -

 下载:
下载:

 点击查看大图
点击查看大图
图(3)
计量
- 文章访问数: 127
- HTML全文浏览量: 27
- PDF下载量: 5
- 被引次数: 0












