 作者投稿
作者投稿 专家审稿
专家审稿 编辑办公
编辑办公 邮件订阅
邮件订阅 RSS
RSS

-
摘要:
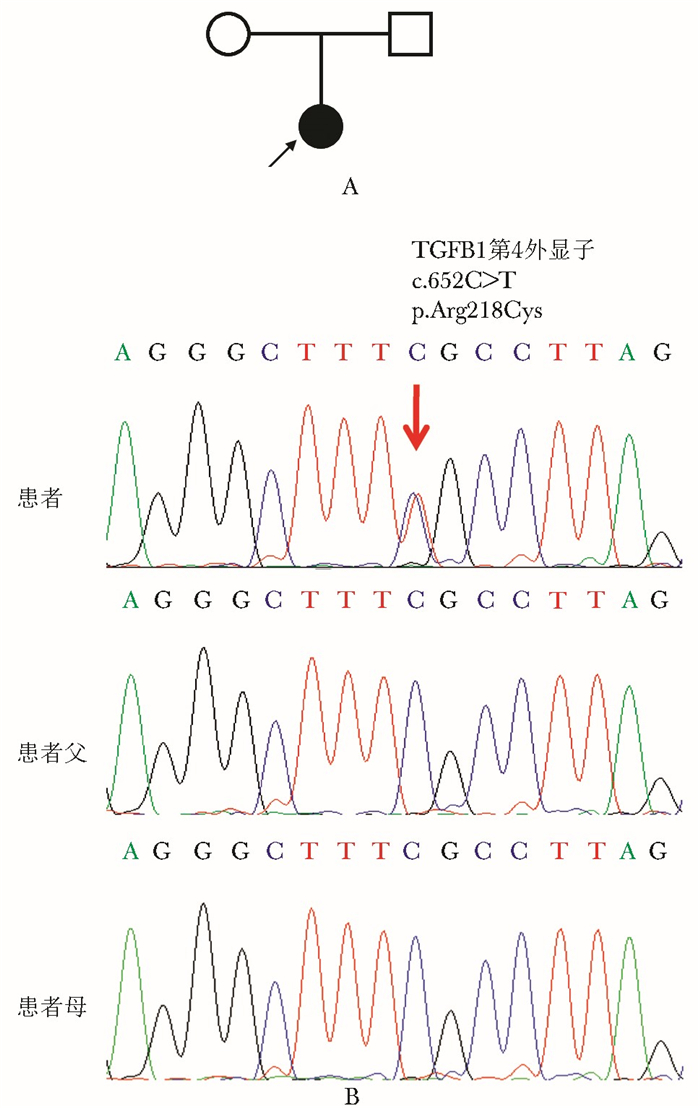
目的 分析1个进行性骨干发育不良(progressive diaphyseal dysplasia, PDD)家系患者的临床表型, 并检测转化生长因子β1编码基因TGFB1的突变类型。 方法 1例幼年起病, 表现为下肢骨痛、无力和肌肉减少的PDD患者, 来自非近亲婚配家庭, 评估其临床表现、骨骼X线特点、骨转换生化指标水平; 采用聚合酶链式反应及其产物直接Sanger测序法检测TGFB1突变。 结果 患者骨转换水平增高, 影像学提示患者四肢骨皮质不均匀性增厚、硬化。基因检测提示患者TGFB1基因第4外显子存在c.652C > T杂合性错义突变(p.Arg218Cys), 患儿父母均未发现该突变。予患者糖皮质激素治疗, 治疗4个月后患者骨痛缓解、活动能力明显改善。 结论 四肢骨痛和骨干皮质增厚是PDD的典型临床表现, TGFB1第218位点错义突变为PDD热点致病突变类型, 糖皮质激素治疗能够缓解PDD病情。 Abstract:Objective To investigate the phenotypes of a kindred with progressive diaphyseal dysplasia (PDD) and to detect the mutation of transforming growth factor beta-1 (TGFB1) gene. Methods A PDD patient of a non-consanguineous family presented with early onset in childhood, who suffered from lower limb pain, fatigability and muscle weakness. Her clinical manifestations, features of skeletal X-ray examination, and bone turnover markers were evaluated. Mutation of TGFB1 was identified by direct Sanger sequencing of polymerase chain reaction amplification product. Results The proband presented with elevated bone turnover biomarkers, and nonuniform thickening and sclerosis of bone cortex of limbs in X-ray films. A heterozygous missense mutation c.652C > T(p.Arg218Cys) in exon 4 of TGFB1 was identified in the proband, but not in either of her parents. Glucocorticoid was given and after 4 months of treatment, the bone pain and activity were obviously improved. Conclusions The typical clinical manifestations of PDD are limb pain and diaphyseal hyperostosis. The missense mutations at position 218 of TGFB1 are hotspot pathogenic mutations of PDD. Glucocorticoids can mitigate the symptoms in PDD patients. -
Key words:
- progressive diaphyseal dysplasia /
- phenotype /
- TGFB1 gene /
- mutation
-

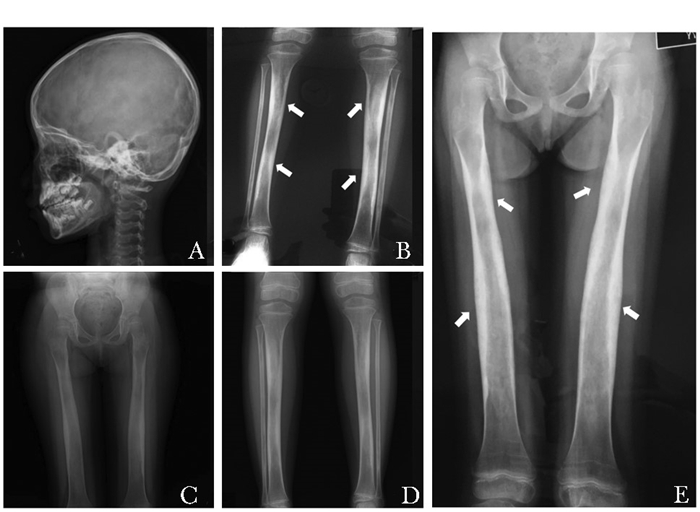
图 2 进行性骨干发育不良患者的影像学表现
A.头颅侧位未见异常;B、E.治疗前患者股骨、胫腓骨骨干增粗,骨皮质不均匀增厚,骨小梁粗乱,相应骨髓腔变窄;C、D.治疗后患者股骨、胫腓骨表现未进一步加重
表 1 TGFB1基因PCR扩增引物序列
外显子 引物名称 引物序列(5′→3′) 长度(bp) 退火温度(℃) 产物长度(bp) Exon 1 TGFB1-1F FCCCACGCGAGATGAGGAC 18 63 1464 TGFB1-1R GCCAGTTTCTTCTGCCAGTC 20 Exon 2 TGFB1-2F GAGACTGACTCCACCCCAGA 20 61 334 TGFB1-2R TTGGTCACAGCTCACCCTCT 20 Exon 3 TGFB1-3F GGTGGCTGTCTGAGAGGGTA 20 60 349 TGFB1-3R GAGAGGGGTCCTAGGCAAAG 20 Exon 4 TGFB1-4F GGTTTGCTCCTTCCTTCCTC 20 60 306 TGFB1-4R AGTGAACCCTGCTTTGGTGT 20 Exon 5 TGFB1-5F CGCCCCACTTATCTATCCCTC 21 60 379 TGFB1-5R TCTTACACCCAGACCTCATCCC 22 Exon 6 TGFB1-6F GGGCATGTGGCTTCTATGGTGG 22 58 276 TGFB1-6R CCTCTTCCTCCGTCCTGGCTC 21 Exon 7 TGFB1-7F GACAGGTGGGGAGAGACAGA 20 60 957 TGFB1-7R CTGGTCTCAAATGCCTGGAT 20  下载: 导出CSV
下载: 导出CSV
表 2 进行性骨干发育不良患者治疗前后的临床特征
时间 年龄(岁) 身高(cm) 体重(kg) Ca(mmol/L) P(mmol/L) ALP(U/L) β-CTX(ng/ml) 25OHD(nmol/L) PTH(ng/L) Cr(μmol/L) ALT(U/L) LS-BMD(g/cm2)* FN-BMD(g/cm2)* TH-BMD(g/cm2)* 治疗前 7.1 118(-1SD) 16(-3SD) 2.31 1.49 200 1.20 23 8.7 31 13 0.673 (+1.2SD) 0.489(-2.3SD) 0.506 治疗后2个月 7.2 118(-1SD) 21(-1SD) 2.47 1.37 193 0.47 46 13.7 28 18 - - - 治疗后4个月 7.3 120(-1SD) 23(中位数) 2.50 1.53 185 0.84 / / 32 14 - - - SD:标准差;Ca:血钙;P:血磷;ALP:碱性磷酸酶;β-CTX:β胶原降解产物;25OHD:25羟维生素D;PTH:甲状旁腺素;Cr:肌酐;ALT:谷丙转氨酶;LS-BMD:腰椎骨密度;FN-BMD:股骨颈骨密度;TH-BMD:全髋骨密度;*由于目前治疗时间较短,治疗后骨密度尚未复查
下载: 导出CSV
-
[1] Bhadada SK, Sridhar S, Steenackers E, et al. Camurati-Engelmann disease (progressive diaphyseal dysplasia):reports of an Indian kindred[J]. Calcif Tissue Int, 2014, 94:240-247. doi: 10.1007/s00223-013-9804-9 [2] Janssens K, Vanhoenacker F, Bonduelle M, et al. Camurati-Engelmann disease:review of the clinical, radiological, and molecular data of 24 families and implications for diagnosis and treatment[J]. J Med Genet, 2006, 43:1-11. http://www.ncbi.nlm.nih.gov/pubmed/15894597 [3] Whyte MP, Totty WG, Novack DV, et al. Camurati-Engelmann disease:unique variant featuring a novel mutation in TGF-beta1 encoding transforming growth factor beta 1 and a missense change in TNFSF11 encoding RANK ligand[J]. J Bone Miner Res, 2011, 26:920-933. doi: 10.1002/jbmr.283 [4] Wu S, Liang S, Yan Y, et al.A novel mutation of TGF-beta1 in a Chinese family with Camurati-Engelmann disease[J]. Bone, 2007, 40:1630-1634. doi: 10.1016/j.bone.2007.02.025 [5] Carlson ML, Beatty CW, Neff BA, et al. Skull base manifestations of Camurati-Engelmann disease[J]. Arch Otolaryngol Head Neck Surg, 2010, 136:566-575. doi: 10.1001/archoto.2010.68 [6] Khadilkar AV, Sanwalka NJ, Chiplonkar SA, et al. Normative data and percentile curves for Dual Energy X-ray Absorptiometry in healthy Indian girls and boys aged 5-17 years[J]. Bone, 2011, 48:810-819. doi: 10.1016/j.bone.2010.12.013 [7] Kinoshita A, Saito T, Tomita H, et al. Domain-specific mutations in TGFB1 result in Camurati-Engelmann disease[J]. Nat Genet, 2000, 26:19-20. doi: 10.1038/79128 [8] Wang C, Zhang BH, Liu YJ, et al. Transforming growth factor-beta1 gene mutations and phenotypes in pediatric patients with Camurati-Engelmann disease[J]. Mol Med Rep, 2013, 7:1695-1699. doi: 10.3892/mmr.2013.1367 [9] Walton KL, Makanji Y, Chen J, et al. Two distinct regions of latency-associated peptide coordinate stability of the latent transforming growth factor-beta1 complex[J]. J Biol Chem, 2010, 285:17029-17037. doi: 10.1074/jbc.M110.110288 [10] Tang Y, Wu X, Lei W, et al. TGF-beta1-induced migration of bone mesenchymal stem cells couples bone resorption with formation[J]. Nat Med, 2009, 15:757-765. doi: 10.1038/nm.1979 [11] Shi M, Zhu J, Wang R, et al. Latent TGF-beta structure and activation[J]. Nature, 2011, 474:343-349. doi: 10.1038/nature10152 [12] Janssens K, Ten DP, Ralston SH, et al. Transforming growth factor-beta 1 mutations in Camurati-Engelmann disease lead to increased signaling by altering either activation or secretion of the mutant protein[J]. J Biol Chem, 2003, 278:7718-7724. doi: 10.1074/jbc.M208857200 [13] Chen G, Deng C, Li YP. TGF-beta and BMP signaling in osteoblast differentiation and bone formation[J].Int J Biol Sci, 2012, 8:272-288. doi: 10.7150/ijbs.2929 [14] Zamani N, Brown CW. Emerging roles for the transforming growth factor-beta superfamily in regulating adiposity and energy expenditure[J]. Endocr Rev, 2011, 32:387-403. doi: 10.1210/er.2010-0018 [15] Toumba M, Neocleous V, Shammas C, et al. A family with Camurati-Engelman disease:the role of the missense p.R218C mutation in TGFbeta1 in bones and endocrine glands[J]. J Pediatr Endocrinol Metab, 2013, 26:1189-1195. [16] Iba K, Takada J, Kamasaki H, et al. A significant improvement in lower limb pain after treatment with alendronate in two cases of Camurati-Engelmann disease[J]. J Bone Miner Metab, 2008, 26:107-109. doi: 10.1007/s00774-007-0783-7 [17] Savoie A, Gouin F, Maugars Y, et al. Treatment responses in five patients with Ribbing disease including two with 466C>T missense mutations in TGFbeta1[J]. Joint Bone Spine, 2013, 80:638-644. doi: 10.1016/j.jbspin.2013.01.007 [18] Trombetti A, Cortes F, Kaelin A, et al. Intranasal calcitonin reducing bone pain in a patient with Camurati-Engelmann disease[J]. Scand J Rheumatol, 2012, 41:75-77. doi: 10.3109/03009742.2011.608195 [19] Castro GR, Appenzeller S, Marques-Neto JF, et al. Camurati-Engelmann disease:failure of response to bisphosphonates:report of two cases[J]. Clin Rheumatol, 2005, 24:398-401. doi: 10.1007/s10067-004-1056-7 [20] Ayyavoo A, Derraik JG, Cutfield WS, et al. Elimination of pain and improvement of exercise capacity in Camurati-Engelmann disease with losartan[J]. J Clin Endocrinol Metab, 2014, 99:3978-3982. doi: 10.1210/jc.2014-2025 [21] Simsek-Kiper PO, Dikoglu E, Campos-Xavier B, et al. Positive effects of an angiotensin Ⅱ type 1 receptor antagonist in Camurati-Engelmann disease:a single case observation[J]. Am J Med Genet A, 2014, 164A:2667-2671. http://www.ncbi.nlm.nih.gov/pubmed/25099136 -

 点击查看大图
点击查看大图
图(3) / 表(2)
计量
- 文章访问数: 290
- HTML全文浏览量: 99
- PDF下载量: 17
- 被引次数: 0












