 作者投稿
作者投稿 专家审稿
专家审稿 编辑办公
编辑办公 邮件订阅
邮件订阅 RSS
RSS

Optic Canal Fracture Evaluation Using Three-Dimensional Computed Tomography Reconstructions
-
摘要:
目的 探讨应用高分辨CT影像学重建技术评价视神经管骨折的可行性。 方法 对1只京豺犬的双侧视神经管在去除软组织后选取16个解剖标志点, 由两个观察者独立测量; 利用16层螺旋CT采用0.10 mm间隔进行重建性扫描, 根据一侧视神经管的解剖学形态, 选取合适的CT重建阈值参数, 包括多平面重建技术(multi-planar reconstruction, MPR)、表面重建技术(surface rendering technique, SRT)、容积再现技术(volume rendering technique, VRT)、空间处理重建技术(InSpace)的窗宽、窗位、明亮度、透度、厚度等, 使得重建的CT影像与实际形态相符。利用该参数系统对所有观察者间一致性高的测量点采用旋转平面投影法进行CT下的空间测量, 结果与解剖学测量值进行比较。对9只京豺犬双侧视神经管按照常见骨折类型(包括撕脱骨折、青枝骨折、分离骨折、塌陷骨折、粉碎骨折)制作骨折模型, 应用前述阈值参数系统, 分别使用被遮表面显示法(surface shaded display, SSD)、最大强度投影(maximum intensity projection, MIP)、VRT和InSpace共4种重建显示技术进行重建, 结果与视神经管正常解剖形态和骨折形态进行比较。利用仿真内窥镜(virtual endoscopy, VE)技术对视神经管骨折的CT影像进行二次重建, 并与形态学结果进行比较。 结果 InSpace三维CT重建技术结合旋转平面投影法测量各径线空间长度, 是一种可靠的量化手段。应用该技术的测量结果与解剖学测量结果相比, 差异无统计学意义(P=1.00)。SSD、VRT、InSpace技术均可以反映视神经管的整体空间形态, 但在不同的骨折类型, 各重建方法的敏感性(对骨折模型的显示程度)和准确性(辨别骨折的具体形态)有差异。InSpace重建模式对多数骨折类型均有较好的显示效果, 但是对塌陷性骨折的整体显示效果差于SSD。SSD技术对于如塌陷性骨折显示效果良好, 而对于明显移位的锐性骨折片显示效果逊于InSpace和VRT。MIP重建法显示各类骨折的效果均不理想。VRT重建法的整体显示骨折的效果介于InSpace和SSD之间。结合MPR重建技术, 可以提高诊断骨折的敏感性。VE技术可以清晰地显示视神经管的内部形态改变, 并对骨折进行较好的鉴别, 所得影像的空间效果感及表面的起伏立体感十分明显。 结论 新一代多层CT扫描及重建技术是一种可行的视神经管骨折诊断手段。通过不同重建方法的综合运用, 可以满足视神经管骨折的三维评价。 Abstract:Objective To investigate the advantage and feasibility of three-dimensional computed tomography (CT) reconstruction technique for optic canal fracture evaluation. Methods After the removal of soft tissues, 16 anatomical markers were selected from the optic canals of one Jackal dog for measurement. One ophthalmologist and one radiologist carried out the measurement independently. The 16-planar spiral CT (Sensation 16, Siemens) was adopted for CT reconstruction, using the interval of 0.1 mm. Reconstructive threshold series was built up based on anatomical results of one optic canal. The threshold series included width, level, brightness, opacity, and thickness et al, during multi-planar reconstruction (MPR), surface rendering technique (SRT), volume rendering technique (VRT), and InSpace technique. According to the threshold series from above, CT spatial measurement was made for all the measuring points agreed between two observers. Rotational projection method was used for measuring. According to common types, fracture models were made from 18 optic canals (9 Jackal dogs), including tear fracture, greenstick fracture, rupture fracture, sink fracture, and comminuted fracture. Surface shaded display (SSD), maximum intensity projection (MIP), VRT and InSpace techniques were applied in CT reconstruction. Comparison was made between the CT reconstruction result and the anatomy of the fracture models. CT virtual endoscopy (VE) technique was applied to reconstruct and fly through the optic canal dynamically, so as to evaluate the recurrence of three-dimensional anatomy. Results InSpace technique combined with the rotating planar projection was a reliable method to measure the length of diameter line in space quantitatively. The measurement results using this method showed no significant difference with the anatomical measurement results (P=1.00). The whole spatial morphology of optic canal could be exhibited by SSD, VR, and InSpace technique. The sensitivity and accuracy of each technique were different depending on the fracture type. InSpace technique showed good result for most fracture types, except the sink fracture. SSD was excellent in displaying the sink fracture, although it presented worse for the sharp fracture compared with InSpace and VRT. MIP was not satisfactory in displaying most fracture types. VRT generally appeared to be the medium between InSpace and SSD in displaying optic canal fracture. Three-dimensional reconstruction combined with MPR remarkably improved the sensitivity for detection of fracture. VE technique presented the inner structure of optic canal clearly. Moreover, it could differentiate between fracture and variation. The effect of VE reconstruction was excellent in terms of spatial appearance and topography. Conclusion Volume CT scanning and three-dimensional reconstruction technique is a reliable diagnostic method. The combination of different reconstructive methods can effectively evaluate the optic canal fracture. -
Key words:
- optic canal /
- computed tomography /
- three-dimensional reconstruction /
- virtual endoscopy
-

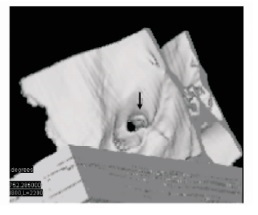
图 7 基于SSD的动态VE过程中截取的CT影像:左侧小撕脱骨折的视神经管前后观(观察点位于眼眶开口处), 骨折片的隆起撕脱和移位均可清晰显示, 立体感强烈(箭头); 骨折撕脱片直径0.4mm
SSD:同图 4; VE:仿真内窥镜

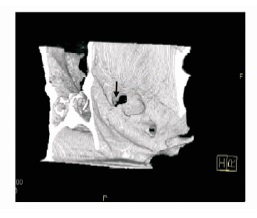
图 8 基于VRT的动态VE过程中截取的CT影像:左侧小撕脱骨折的视神经管前后观(观察点接近于撕脱处), 可清晰显示骨折撕脱片(箭头), 直径0.4mm
VRT:容积再现技术; VE:同图 7
表 1 观察者之间对所有解剖测量点的一致性检验结果($\bar x \pm s$)

-
[1] 胡福广, 张庆俊.中国人视神经管显微解剖学研究[J].中国神经精神疾病杂志, 2001, 27:119-121. http://www.wanfangdata.com.cn/details/detail.do?_type=perio&id=zgsjjsjbzz200102013 [2] 宋维贤, 孙华.不同入路视神经管减压开放术疗效分析[J].眼科, 2002, 11:286-288. http://www.wanfangdata.com.cn/details/detail.do?_type=perio&id=yk200205008 [3] 田继辉, 于春江, 孙涛.视神经管及眶上裂区巨微解剖学研究[J].中国临床解剖学研究, 1999, 17:275-277. http://www.wanfangdata.com.cn/details/detail.do?_type=perio&id=QK199901141698 [4] Attia M, Kandasamy J, Jakimovski D, et al. The importance and timing of optic canal exploration and decompression during endoscopic endoasal resection of tuberculum sella and planum sphenoidale meningiomas[J]. Neurosurgery, 2012, 71(1 Suppl Operative):58-67. http://www.ncbi.nlm.nih.gov/pubmed/22517253 [5] Yang QT, Zhang GH, Liu X, et al. The therapeutic efficacy of endoscopic optic nerve decompression and its effects on the prognoses of 96 cases of traumatic optic neuropathy[J]. J Trauma Acute Care Surg, 2012, 72:1350-1355. doi: 10.1097/TA.0b013e3182493c70 [6] Bartolozzi C. 3D Image Processing[M]. Berlin:Springer, 2001. [7] 杨钦泰, 李源, 邹艳, 等.计算机辅助视神经管三维立体定位的CT影像学研究[J].临床耳鼻喉头颈外科杂志, 2008, 22:306-308, 311. http://www.wanfangdata.com.cn/details/detail.do?_type=perio&id=lcebyhkzz200807007 [8] Neubauer A, Wolfsberger S. Virtual endoscopy in neurosurgery:a review[J]. Neurosurgery, 2013, 72(suppl 1):A97-A106. doi: 10.1227/neu.0b013e31827393c9 [9] Våpenstad C, Buzink SN. Procedural virtual reality simulation in minimally invasive surgery[J]. Surg Endosc, 2013, 27:364-377. doi: 10.1007/s00464-012-2503-1 -

 下载:
下载:





 点击查看大图
点击查看大图

图(8) / 表(1)
计量
- 文章访问数: 132
- HTML全文浏览量: 27
- PDF下载量: 8
- 被引次数: 0












