 作者投稿
作者投稿 专家审稿
专家审稿 编辑办公
编辑办公 邮件订阅
邮件订阅 RSS
RSS

-
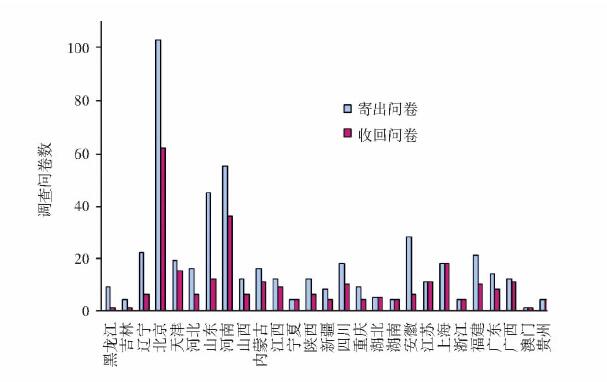
摘要:
目的 针对我国气道管理的现状进行问卷调查, 为改进和完善我国气道管理提供参考。 方法 采用邮寄调查问卷的方法, 对全国27个省市自治区78家医院进行调查。调查问卷包括被调查者基本情况, 对各种气道工具的熟知和使用程度, 对临床几种气道情景的处理以及科室气道管理等4个部分。以教学和非教学医院为分组变量, 采用校正χ2检验进行分析比较。 结果 调查问卷有效回收率为60.7%。所有麻醉医师最熟悉且能熟练使用的是Macintosh喉镜片、标准镜柄、口咽通气道和塑形管芯。教学医院麻醉医师对视频喉镜Glidescope、可视管芯、插管型喉罩及纤维支气管镜的了解和熟练使用与非教学医院比较差异有显著统计学意义(P < 0.01)。对其他气道工具, 包括紧急气道工具的了解和使用教学与非教学医院差异较大。对有明确插管困难的患者, 近半数麻醉医师(46.9%)选择纤维支气管镜下清醒插管; 79.2%的麻醉医师遇到意外插管困难时能在维持通气时尝试其他方法; 遇到不能通气不能插管时, 首选喉罩改善通气和环甲膜穿刺建立气道的麻醉医师分别为47.6%和52.4%;怀疑有插管困难, 绝大多数麻醉医师(92.6%)会先尝试麻醉后直接喉镜插管。教学医院在建立简便气道处理流程、专业团队建设和培训上比非教学医院好(P < 0.01)。 结论 被调查的麻醉医师对气道管理工具的认识和使用差异较大, 但对气道处理流程的遵循较好。麻醉科室在气道管理方面仍有需改善之处。 Abstract:Objective To perform a preliminary survey on airway management in China. Methods The postal questionnaires were sent to anesthesiologists in 78 hospitals of 27 provinces/municipalities/autonomous regions. The questionnaire contained four parts which included the general information of respondents, the knowledge and usage of various airway tools, the practical patterns to different clinical airway scenarios, and the administrative management of the anesthesiology department. Chi-square analysis was performed for categorical variable (teaching hospital or non-teaching hospital). Results The response rate was 60.7%. Direct laryngoscope using Macintosh blade with standard handle, oral airway, and malleable stylet were the most familiar airway tools for all the respondents. Anesthesiologists in teaching hospitals had better knowledge and more frequent usage of Glidescope, seeing stylet, intubating laryngeal mask airway, and fiberoptical bronchoscope than those in non-teaching hospitals (P < 0.01). There were large variations between teaching and non-teaching hospitals in the knowledge and usage for other airway tools including emergency tools. Nearly half of respondents (46.9%) preferred to choose awake fiberopitcal intubation as their first choices for definite difficult intubation patients. When encountering unexpected difficult intubation, 79.2% of anesthesiologists would attempt alternative tools to intubate only if they could maintain the airway. For patients who were unable to be intubated or ventilated, 47.6% of the responders preferred to improve ventilation using larngeal mask airway as first choice while 52.4% preferred to establish an emergency airway via cricothyrotomy. For suspected difficult intubation, most respondents (92.6%) would attempt to paralyze patient and intubate with direct laryngoscopy. Teaching hospitals were better than nonteaching hospitals in terms of establishing simple airway management algorithm, subspecialty development, and staff training (P < 0.01). Conclusions Although the knowledge and usage of airway tools differ among anesthesiologists in China, most of them well follow the airway management algorithm in different airway scenarios. However, the administrative management of the anesthesiology department requires further improvement. -
Key words:
- airway management /
- questionnaire survey
-
表 1 有效问卷麻醉医师基本情况
项目 人数 % 性别 男 175 58. 7 女 123 41. 3 工作年限 0 ~ 3 47 15. 8 (年) 4 ~ 8 73 24. 5 9 ~ 15 90 30. 2 >15 88 29. 5 医院级别 省市级以上教学医院 107 35. 9 市级非教学医院 146 49. 0 区级医院 43 14. 4 其他 2 0. 7 所属科室 麻醉科 275 92. 3 ICU 4 1. 3 麻醉科 & ICU 19 6. 4 ICU:重症监护病房  下载: 导出CSV
下载: 导出CSV
表 2 麻醉医师对气道管理工具的了解与使用(%)
气道管理工具 了解 熟练使用 直接喉镜 Macintosh镜片 100. 0 100. 0 Miller镜片 84. 0 8. 3 标准手柄 100. 0 100. 0 短柄手柄 14. 3 0 改良喉镜 McCoy 13. 5 2. 3 硬质喉镜 20. 2 0 视频喉镜 34. 2 16. 1 管芯 塑型 100. 0 100. 0 探条(bougie) 27. 6 8. 4 光棒 41. 3 12. 4 可视管芯 27. 2 11. 4 纤维支气管镜 99. 7 24. 2 口咽通气道 100. 0 100. 0 鼻咽通气道 97. 2 20. 8 喉罩 100. 0 经典 21. 9 36. 2 双管 73. 1 48. 1 插管型 16. 8 6. 7 食管-气管联合导管 10. 7 0 换管器 13. 5 0 高频通气 98. 3 7. 6 逆行插管套装 93. 2 0 环甲膜切开套装 86. 3 0 气管切开套装 100. 0 0
下载: 导出CSV
表 3 教学与非教学医院麻醉医师对4种气道工具了解和熟练使用比较(%)
气道工具 了解 熟练使用 总和 非教学医院 教学医院 总和 非教学医院 教学医院 可视喉镜 34. 2 40. 2 59. 8* 16. 1 39. 6 60. 4* 可视管芯 27. 2 42. 0 58. 0* 11. 4 44. 1 55. 9* 插管型喉罩 16. 8 38. 0 62. 0* 6. 7 15. 0 85. 0* 纤维支气管镜 99. 7 - - 24. 2 18. 1 81. 9* - :未填写; 与非教学医院比较,* P<0. 01
下载: 导出CSV
表 4 气道管理的科室建设和管理(%)
项目 非教学医院 教学医院 总和 设立困难气道车 0. 6 2. 0 1. 1 建立困难气道处理简易流程 44. 6 72. 7* 55. 1 专业团队建设 3. 0 12. 1* 6. 4 继续教育 培训计划和参加学习班 33. 7 70. 7* 47. 5 培训演练和用具 15. 7 35. 3* 23. 0 病例报告及讨论 71. 2 81. 8 75. 1 与非教学医院比较,* P<0. 01
下载: 导出CSV
-
[1] Wong DT, Lai K, Chung FF, et al. Cannot intubate-cannot ventilate and difficult intubation strategies:results of a Canadian national survey[J]. Anesth Analg, 2005, 100:1439-1446. doi: 10.1213/01.ANE.0000148695.37190.34 [2] Rosenblatt WH, Wagner PJ, OVassapian A, et al. Practice patterns in managing the difficult airway by anesthesiologists in the United States[J]. Anesth Analg, 1998, 87:153-157. http://www.ncbi.nlm.nih.gov/pubmed/9661565 [3] Marco CA, Marco AP. Airway adjuncts[J]. Emerg Med Clin N Am, 2008, 26:1015-1027. doi: 10.1016/j.emc.2008.07.005 [4] Frova G, Sorbello M. Algorithms for difficult airway management:a review[J]. Minerva Anesthesiol, 2009, 75:201-209. http://www.ncbi.nlm.nih.gov/pubmed/18946426 [5] McIntyre JWR. Laryngoscope design and the difficult adult tracheal intubation[J]. Can J Anaesth, 1989, 36:94-98. doi: 10.1007/BF03010896 [6] Mellado PF, Thunedborg LP, Swiatek F, et al. Anaesthesiological airway management in Denmark:Assessment, equipment and documentation[J]. Acta Anaesthesiol Scand, 2004, 48:350-354. doi: 10.1111/j.0001-5172.2004.0337.x [7] Dimitriou V, Iatrou C, Douma A, et al. Airway management in Greece:a nationwide postal survey[J]. Minerva Anesthesiol, 2008, 74:453-458. http://www.ncbi.nlm.nih.gov/pubmed/18762752 [8] Jenkins K, Wong DT, Correa R. Management choices for the difficult airway by anesthesiologists in Canada[J]. Can J Anesth, 2002, 49:850-856. doi: 10.1007/BF03017419 [9] Goldmann K, Braun U. Airway management practices at German university and university-affiliated teaching hospitals; equipment, techniques and training:results of a nationwide survey[J]. Acta Anaesthesiol Scand, 2006, 50:298-305. doi: 10.1111/j.1399-6576.2006.00853.x [10] 赵欣, 田鸣, 李树人.新型可视纤维气管镜用于困难气道气管内插管[J].中国医刊, 2008, 43:57-58. http://www.wanfangdata.com.cn/details/detail.do?_type=perio&id=zgyk200812023 [11] Borg PA, Stuart C, Dercksen B, et al. Anesthetic management of the airway in the Netherlands:a postal survey[J]. Eur J Anesthesiol, 2001, 18:73-78. doi: 10.1046/j.1365-2346.2001.00908.x/pdf [12] Myneni N, O'Leary MA, Sandison M, et al. Evaluation of the upper bite test in predicting difficult laryngoscopy[J]. J Clin Anesth, 2010, 22:174-178. doi: 10.1016/j.jclinane.2009.06.004 [13] 田鸣, 邓晓明, 朱也森, 等.困难气道管理专家共识[J].临床麻醉学, 2009, 25:200-203. http://www.wanfangdata.com.cn/details/detail.do?_type=perio&id=lcmzxzz200903005 [14] Ezri T, Szmuk P, Warters RD, et al. Diffficult airway management practice patterns among anesthesiologists practicing in the Unite States:Have we make any progress?[J]. J Clin Anesth, 2003, 15:418-422. doi: 10.1016/S0952-8180(03)00080-1 [15] Barash PG, Cullen BF, Stoelting RK. Clinical anesthesia[M]. 4th ed. Philiadelphia: Lippincott Williams & Wilkin, 2001: 614-615. [16] Parmet JL, Colomma-Romano P, Horrow JC, et al. The laryngeal mask airway reliably provides rescue ventilation in cases of unanticipated difficult tracheal intubation along with difficult mask ventilation[J]. Anesth Analg, 1998, 87:661-665. http://www.ncbi.nlm.nih.gov/pubmed/9728849 [17] Abrishami A, Zilbernan P, Chung F. Airway rescue with insertion of laryngeal mask airway devices with patients in the prone position[J]. Can J Anaesth, 2010, 57:1014-1020. doi: 10.1007/s12630-010-9378-1 [18] Benumof JL. Management of the difficult adult airway[J]. Anesthesiology, 1991, 75:1087-1110. doi: 10.1097/00000542-199112000-00021 [19] Barker PA, Flanagean BT, Greenland KB, et al. Equipment to manage a difficult airway during anaesthesia[J]. Anaesth Intensive Care, 2011, 59:16-34. http://www.ncbi.nlm.nih.gov/pubmed/21375086 [20] Porhomayon J, EI-Solh AA, Nader ND. National survey to assess the content and availability of difficult airway carts in critical care units in the Unite States[J]. J Anesth, 2010, 24:811-814. doi: 10.1007/s00540-010-0996-0 [21] Stamer UM, Messerschmidt A, Wulf H, et al. Equipment for the difficult airway in obstetric units in Germany[J]. J Clin Anesth, 2000, 12:151-156. doi: 10.1016/S0952-8180(00)00131-8 [22] Stringer KR, Bejenov S, Yentis SM. Training in airway management[J]. Anaesthesia, 2002, 57:967-983. doi: 10.1046/j.1365-2044.2002.02830.x -

 点击查看大图
点击查看大图
图(1) / 表(4)
计量
- 文章访问数: 267
- HTML全文浏览量: 97
- PDF下载量: 7
- 被引次数: 0












