 作者投稿
作者投稿 专家审稿
专家审稿 编辑办公
编辑办公 邮件订阅
邮件订阅 RSS
RSS

Cronkhite-Canada Syndrome Combined with Asymptomatic Novel Coronavirus Infection: A Case Report
-
摘要: 本文报道Cronkhite-Canada综合征合并无症状新型冠状病毒感染1例。该患者临床表现为食欲减退,毛发及指甲脱落,皮肤色素沉着。内镜检查见胃、十二指肠及结肠黏膜呈弥漫性、大小不一、密集分布的息肉样改变。病程中检出新型冠状病毒核酸阳性。经中等剂量泼尼松治疗后,患者毛发恢复生长,皮肤色素沉着减退。本文总结该患者的诊疗经过并结合文献复习,以期提升临床医生对该病的认知。
-
关键词:
- Cronkhite-Canada综合征 /
- 新型冠状病毒感染 /
- 治疗
Abstract: This article presents a case study of a patient who had Cronkhite-Canada syndrome in combination with an asymptomatic novel coronavirus infection. The patient exhibited clinical symptoms of loss of appetite, hair and nail loss, and skin pigmentation. Digestive endoscopy revealed widespread and varying-sized polypoid changes in the mucosa of the stomach, duodenum, and colon. During the course of the illness, the patient tested positive for novel coronavirus nucleic acid. Treatment with moderate doses of prednisone resulted in the patient's hair regrowth and decreased skin hypopigmentation. The article provides a summary of the patient's diagnosis and treatment and a review of relevant literature, with the aim of enhancing clinicians' understanding of the disease.-
Key words:
- Cronkhite-Canada syndrome /
- novel coronavirus infection /
- treatment
作者贡献:张宁、杨晨皓负责病例整理、论文撰写及修订;孙晓红负责论文构思及修订;周良瑞提供患者病理图片;康琳、刘晓红、李骥、李海龙提供诊疗思路。利益冲突:所有作者均声明不存在利益冲突注:本研究发表已征得患者知情同意。 -

图 1 患者发病前后身体毛发变化
A.发病前(2023年2月)毛发正常;B.入院时头发、眉毛、胡须脱落;C.入院时睫毛变长并弯曲上翘;D.入院时双手指甲呈黄白色且部分脱落;E.入院时双手掌色素沉着
Figure 1. The changes in body hair of the patient before and after the onset of the disease
A.Prior to the onset of the disease (February 2023), the hair appeared normal; B.Upon admission, the patient experienced hair loss, including eyebrows and beards; C.The patient's eyelashes became longer and curved upwards; D.The patient lost the nails on both hands, which appeared yellowish white and partially peeled off; E.There was pigmentation observed on both palms upon admission

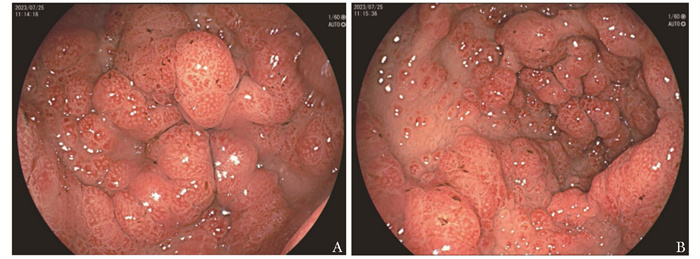
图 2 胃镜检查示胃体下部小弯、胃窦黏膜可见弥漫性、大小不一、密集分布的充血息肉样改变(2023-07-25)
Figure 2. Gastroscopy revealed diffuse congestive polyp-like changes of varying sizes and dense distribution in the mucosa of the lower curvature of the gastric body and the gastric antrum(2023-07-25)

图 3 结肠镜检查示多发无蒂、色红息肉(2023-07-20)
Figure 3. Colonoscopy showed multiple sessile, red polyps(2023-07-20)

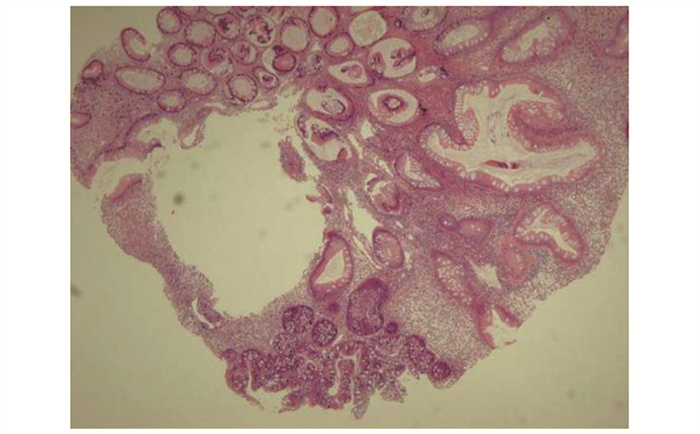
图 4 患者结肠镜下切除息肉病理示错构瘤性息肉,局部伴低级别异型增生(HE,×40)
Figure 4. Pathology of the patient's polyp resection during colonoscopy indicated the presence of hamartomatous polyps with local low-grade dysplasia (HE, ×40)
-
[1] Vashistha N, Chakravarty S, Singhal D. Cronkhite-Canada syndrome[J]. Gastrointest Endosc, 2017, 86(5): 922-923. doi: 10.1016/j.gie.2017.05.028 [2] CRONKHITE L W, Jr, CANADA W J. Generalized gastrointestinal polyposis; an unusual syndrome of polyposis, pigmentation, alopecia and onychotrophia[J]. N Engl J Med, 1955, 252(24): 1011-1015. doi: 10.1056/NEJM195506162522401 [3] Slavik T, Montgomery E A. Cronkhite-Canada syndrome six decades on: the many faces of an enigmatic disease[J]. J Clin Pathol, 2014, 67(10): 891-897. doi: 10.1136/jclinpath-2014-202488 [4] Lu Y Y, Huang F X, Wang Y W, et al. Clinical and endoscopic characteristics of Chinese Cronkhite-Canada syndrome patients: a retrospective study of 103 cases[J]. Dig Dis, 2021, 39(5): 488-495. doi: 10.1159/000514354 [5] Miyawaki K, Komori T, Ishida Y, et al. Cronkhite-Canada syndrome mimicking COVID-19-related symptoms[J]. Acta Derm Venereol, 2022, 102: adv00812. doi: 10.2340/actadv.v102.3402 [6] Yoshimoto T, Okamoto T, Fukuda K. Cronkhite-Canada syndrome: a rare COVID-19 mimicker[J]. Am J Gastroenterol, 2021, 116(8): 1765. doi: 10.14309/ajg.0000000000001254 [7] Øksnes M, Husebye E S. Approach to the patient: diagnosis of primary adrenal insufficiency in adults[J]. J Clin Endocrinol Metab, 2023, 109(1): 269-278. doi: 10.1210/clinem/dgad402 [8] Hashim M, Athar S, Gaba W H. New onset adrenal insufficiency in a patient with COVID-19[J]. BMJ Case Rep, 2021, 14(1): e237690. doi: 10.1136/bcr-2020-237690 [9] Kumar R, Guruparan T, Siddiqi S, et al. A case of adrenal infarction in a patient with COVID 19 infection[J]. BJR Case Rep, 2020, 6(3): 20200075. [10] Siejka A, Barabutis N. Adrenal insufficiency in the COVID-19 era[J]. Am J Physiol Endocrinol Metab, 2021, 320(4): E784-E785. doi: 10.1152/ajpendo.00061.2021 [11] Kanczkowski W, Evert K, Stadtmüller M, et al. COVID-19 targets human adrenal glands[J]. Lancet Diabetes Endocrinol, 2022, 10(1): 13-16. doi: 10.1016/S2213-8587(21)00291-6 [12] Goto A. Cronkhite-Canada syndrome: epidemiological study of 110 cases reported in Japan[J]. Nihon Geka Hokan, 1995, 64(1): 3-14. [13] Murata I, Yoshikawa I, Endo M, et al. Cronkhite-Canada syndrome: report of two cases[J]. J Gastroenterol, 2000, 35(9): 706-711. doi: 10.1007/s005350070051 [14] Ikeda K, Sannohe Y, Murayama H. A case of Cronkhite-Canada syndrome developing after hemi-colectomy[J]. Endoscopy, 1981, 13(6): 251-253. doi: 10.1055/s-2007-1021699 [15] Zong Y, Zhao H Y, Yu L, et al. Case report-malignant transformation in Cronkhite-Canada syndrome polyp[J]. Medicine (Baltimore), 2017, 96(6): e6051. doi: 10.1097/MD.0000000000006051 [16] Wen X H, Wang L, Wang Y X, et al. Cronkhite-Canada syndrome: report of six cases and review of literature[J]. World J Gastroenterol, 2014, 20(23): 7518-7522. doi: 10.3748/wjg.v20.i23.7518 [17] Takeuchi Y, Yoshikawa M, Tsukamoto N, et al. Cronkhite-Canada syndrome with colon cancer, portal thrombosis, high titer of antinuclear antibodies, and membranous glomerulonephritis[J]. J Gastroenterol, 2003, 38(8): 791-795. doi: 10.1007/s00535-002-1148-6 [18] Fan R Y, Wang X W, Xue L J, et al. Cronkhite-Canada syndrome polyps infiltrated with IgG4-positive plasma cells[J]. World J Clin Cases, 2016, 4(8): 248-252. doi: 10.12998/wjcc.v4.i8.248 [19] Watanabe C, Komoto S, Tomita K, et al. Endoscopic and clinical evaluation of treatment and prognosis of Cronkhite-Canada syndrome: a Japanese nationwide survey[J]. J Gastroenterol, 2016, 51(4): 327-336. doi: 10.1007/s00535-015-1107-7 [20] Kato K, Ishii Y, Mazaki T, et al. Spontaneous regression of polyposis following abdominal colectomy and Helicobacter pylori eradication for Cronkhite-Canada syndrome[J]. Case Rep Gastroenterol, 2013, 7(1): 140-146. doi: 10.1159/000350321 [21] Boland B S, Bagi P, Valasek M A, et al. Cronkhite Canada syndrome: significant response to infliximab and a possible Clue to pathogenesis[J]. Am J Gastroenterol, 2016, 111(5): 746-748. [22] Ho V, Banney L, Falhammar H. Hyperpigmentation, nail dystrophy and alopecia with generalised intestinal polyposis: Cronkhite-Canada syndrome[J]. Australas J Dermatol, 2008, 49(4): 223-225. doi: 10.1111/j.1440-0960.2008.00474.x [23] Wu Z Y, Sang L X, Chang B. Cronkhite-Canada syndrome: from clinical features to treatment[J]. Gastroenterol Rep (Oxf), 2020, 8(5): 333-342. doi: 10.1093/gastro/goaa058 [24] 李媛, 罗涵青, 吴东, 等. Cronkhite-Canada综合征临床病理学分析及IgG4阳性浆细胞浸润的意义[J]. 中华病理学杂志, 2018, 47(10): 753-757. Li Y, Luo H Q, Wu D, et al. Clinicopathologic features of Cronkhite-Canada syndrome and the significance of IgG4-positive plasma cells infiltration[J]. Chin J Pathol, 2018, 47(10): 753-757. [25] Wallenhorst T, Pagenault M, Bouguen G, et al. Small-bowel video capsule endoscopic findings of Cronkhite-Canada syndrome[J]. Gastrointest Endosc, 2016, 84(4): 739-740. doi: 10.1016/j.gie.2016.04.004 [26] Murata M, Bamba S, Takahashi K, et al. Application of novel magnified single balloon enteroscopy for a patient with Cronkhite-Canada syndrome[J]. World J Gastroenterol, 2017, 23(22): 4121-4126. doi: 10.3748/wjg.v23.i22.4121 [27] Jha A K, Kumar A, Singh S K, et al. Panendoscopic characterization of Cronkhite-Canada syndrome[J]. Med J Armed Forces India, 2018, 74(2): 196-200. doi: 10.1016/j.mjafi.2017.03.007 [28] Bettington M, Brown I S, Kumarasinghe M P, et al. The challenging diagnosis of Cronkhite-Canada syndrome in the upper gastrointestinal tract: a series of 7 cases with clinical follow-up[J]. Am J Surg Pathol, 2014, 38(2): 215-223. doi: 10.1097/PAS.0000000000000098 [29] Nagata J, Kijima H, Hasumi K, et al. Adenocarcinoma and multiple adenomas of the large intestine, associated with Cronkhite-Canada syndrome[J]. Dig Liver Dis, 2003, 35(6): 434-438. doi: 10.1016/S1590-8658(03)00160-9 [30] Karasawa H, Miura K, Ishida K, et al. Cronkhite-Canada syndrome complicated with huge intramucosal gastric cancer[J]. Gastric Cancer, 2009, 12(2): 113-117. doi: 10.1007/s10120-009-0506-y [31] Watari J, Morita T, Sakurai J, et al. Endoscopically treated Cronkhite-Canada syndrome associated with minute intramucosal gastric cancer: an analysis of molecular pathology[J]. Dig Endosc, 2011, 23(4): 319-323. doi: 10.1111/j.1443-1661.2011.01150.x [32] Maruno T, Kikuyama M. Cronkhite-Canada syndrome associated with sigmoid colon cancer[J]. Clin Gastroenterol Hepatol, 2011, 9(11): e118-e119. doi: 10.1016/j.cgh.2011.06.003 [33] Yuan B S, Jin X X, Zhu R M, et al. Cronkhite-Canada syndrome associated with rib fractures: a case report[J]. BMC Gastroenterol, 2010, 10: 121. doi: 10.1186/1471-230X-10-121 [34] Liu S, Ruan G C, You Y, et al. A striking flail chest: a rare manifestation of intestinal disease[J]. Intest Res, 2019, 17(1): 155-156. doi: 10.5217/ir.2018.00132 [35] Yasuda T, Ueda T, Matsumoto I, et al. Cronkhite-Canada syndrome presenting as recurrent severe acute pancreatitis[J]. Gastrointest Endosc, 2008, 67(3): 570-572. doi: 10.1016/j.gie.2007.07.041 [36] Yun S H, Cho J W, Kim J W, et al. Cronkhite-Canada syndrome associated with serrated adenoma and malignant polyp: a case report and a literature review of 13 Cronkhite-Canada syndrome cases in Korea[J]. Clin Endosc, 2013, 46(3): 301-305. doi: 10.5946/ce.2013.46.3.301 [37] Tong J Y, Wong A, Zhu D, et al. The prevalence of olfactory and gustatory dysfunction in COVID-19 patients: a systematic review and meta-analysis[J]. Otolaryngol Head Neck Surg, 2020, 163(1): 3-11. doi: 10.1177/0194599820926473 [38] Zhu X, Shi H Y, Zhou X N, et al. A case of recurrent Cronkhite-Canada syndrome containing colon cancer[J]. Int Surg, 2015, 100(3): 402-407. doi: 10.9738/INTSURG-D-14-00003.1 [39] Schulte S, Kütting F, Mertens J, et al. Case report of patient with a Cronkhite-Canada syndrome: sustained remission after treatment with corticosteroids and mesalazine[J]. BMC Gastroenterol, 2019, 19(1): 36. doi: 10.1186/s12876-019-0944-x -

 下载:
下载:


 点击查看大图
点击查看大图

计量
- 文章访问数: 49
- HTML全文浏览量: 6
- PDF下载量: 11
- 被引次数: 0












