 作者投稿
作者投稿 专家审稿
专家审稿 编辑办公
编辑办公 邮件订阅
邮件订阅 RSS
RSS

-
摘要: 肾上腺皮质癌(adrenocortical carcinoma,ACC)是发生于肾上腺皮质的罕见恶性肿瘤,手术为其首选治疗方式。对于无法手术切除、肿瘤已发生转移或术后有病灶残留的患者,药物治疗和放疗可作为辅助治疗方式。米托坦是美国食品药品监督管理局和欧洲药品管理局批准的适应证为ACC的唯一药物,其通过抑制线粒体呼吸、引起线粒体相关膜功能障碍及内质网应激等途径减少ACC细胞增殖,同时通过调控多种类固醇激素合成酶的功能和表达水平进而降低ACC细胞分泌功能,是多个国际指南和共识推荐的ACC首选辅助治疗药物。米托坦治疗期间需维持血药浓度在14~20 mg/L之间,监测药物相关不良反应,并警惕与其他药物的相互作用。为促进我国米托坦治疗ACC临床应用进一步规范化,保障用药的有效性和安全性,北京协和医院依托罕见病多学科诊疗团队,组织相关领域专家,经多次讨论、修改,最终制订了本共识,以供临床参考。Abstract: Adrenocortical carcinoma (ACC) is a rare malignant tumor that occurs in the adrenal cortex, and surgery is the first choice for treating ACC. Medical therapy and radiotherapy are adjuvant treatments for patients with unresectable metastasized tumors or incomplete resection. Mitotane is the only adrenergic cytotoxic drug approved by the American Food and Drug Administration and European Medicines Agency for the treatment of ACC by inhibiting mitochondrial respiration, causing mitochondrial membrane dysfunction and inducing endoplasmic reticulum stress, and it reduces the secretory function of ACC cells by inhibiting the function and expression of several enzymes in the adrenocortical steroidogenesis pathway. Mitotane is recommended as the first choice for adjuvant therapy by multiple international guidelines and consensus. During treatment with mitotane, its blood concentration should be maintained between 14 to 20 mg/L, while the related adverse drug reactions and drug-drug interactions should also be monitored. To promote further standardization of the clinical application of mitotane, and to ensure the effectiveness and safety of mitotane, Peking Union Medical College Hospital relied on the multi-disciplinary team for the diagnosis and treatment of rare diseases, organized experts and scholars in related fields to discuss and modify many times, and finally formed this consensus for clinicians' reference.
-
Key words:
- mitotane /
- adrenocortical carcinoma /
- expert consensus /
- rare disease /
- orphan drug
-
表 1 欧洲肾上腺肿瘤研究网定义的肾上腺皮质癌分期[7]
分期 定义 Ⅰ T1,N0,M0 Ⅱ T2,N0,M0 Ⅲ T1~T2,N1,M0 T3~T4,N0~N1,M0 Ⅳ T1~T4,N0~N1,M1 T1:肿瘤最大径≤ 5 cm;T2:肿瘤最大径>5 cm;T3:肿瘤浸润周围组织;T4:肿瘤侵入邻近器官或腔静脉;N0:无阳性淋巴结;N1:存在阳性淋巴结;M0:无远处转移;M1:存在远处转移  下载: 导出CSV
下载: 导出CSV
表 2 米托坦治疗肾上腺皮质癌专家共识推荐意见
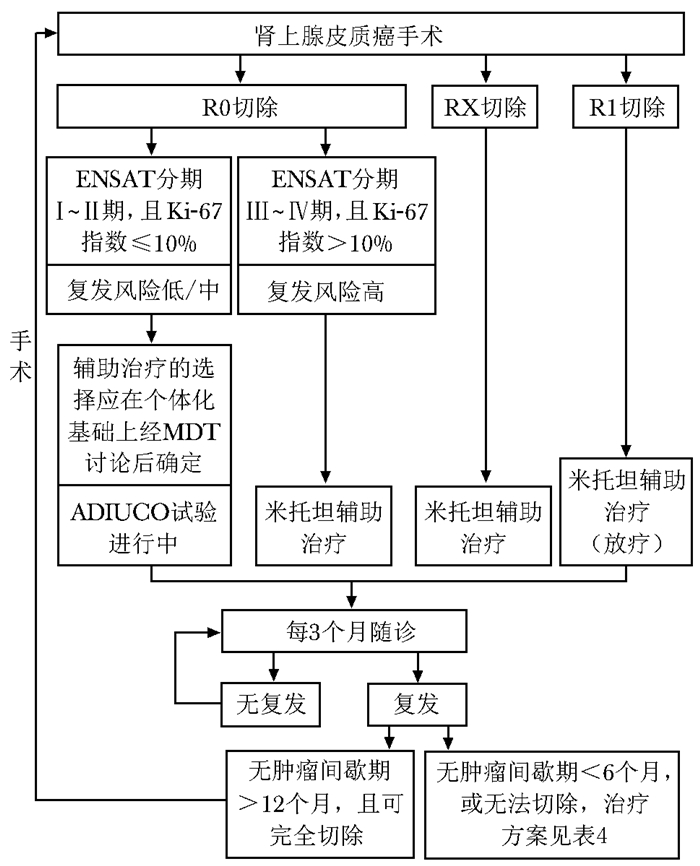
序号 临床问题 推荐意见(证据等级,推荐强度) 1 米托坦治疗的适用人群及其有效性 根治性手术后复发风险高的患者(ENSAT分期Ⅲ~Ⅳ期,或R1~RX切除,或Ki-67指数>10%)应予以米托坦辅助治疗;对于低/中复发风险(ENSAT分期Ⅰ~Ⅱ期,或R0切除,或Ki-67指数≤10%)的患者,辅助治疗的选择应在个体化基础上经MDT讨论后确定(证据等级:2a;推荐强度:B) 对于不能完整手术切除的晚期/复发性ACC,可选择的治疗方式包括射频消融、化学栓塞、放疗及药物治疗等;治疗方案的选择应在个体化基础上经MDT讨论后确定; 根据疾病预后参数,使用米托坦单药治疗或EDP-M方案(依托泊苷、阿霉素和顺铂联合米托坦)治疗;若患者无法耐受EDP-M方案,则采用(E)P-M方案(证据等级:1b;,推荐强度:A) 2 起始治疗方案和剂量调整方案 采用根据患者临床表现及开始用药前几周耐受性逐渐增加米托坦剂量的治疗方案,并根据血药浓度调整用药剂量以达到治疗血药浓度(14~20 mg/L)或最大耐受(证据等级:3b;推荐强度:B) 3 米托坦治疗的起始时间和持续时间 所有具有米托坦治疗适应证的ACC患者,尽快开始米托坦治疗,同时米托坦持续治疗时间至少为2年(证据等级:4;推荐强度:C) 接受米托坦治疗1年后病情进展的患者,在个体化基础上经MDT讨论后确定米托坦停用方案(证据等级:4;推荐强度:C) 4 糖皮质激素及其推荐剂量 在米托坦治疗初期或出现肾上腺功能不全时,所有接受米托坦治疗的患者(皮质醇持续过量者除外)使用糖皮质激素(氢化可的松)替代治疗,并根据24 h尿液游离皮质醇水平和临床体征综合评估氢化可的松用药剂量(本专家共识推荐强度:推荐) 5 米托坦血药浓度监测和剂量调整 所有应用米托坦治疗的ACC患者,均应进行TDM,并根据监测结果调整米托坦用药剂量,使其血药浓度维持在14~20 mg/L的治疗窗内(证据等级:2b;推荐强度:B) 米托坦是CYP3A4的强诱导剂,对于同时服用CYP3A4底物药物的患者,应关注米托坦相关药物的相互作用,监测患者对合用药物剂量变化的反应,并结合临床症状和TDM结果,及时调整药物方案(本专家共识推荐强度:强烈推荐) 6 特殊人群用药及米托坦不良反应的预防处理 在接受米托坦治疗时采取避孕措施;18岁以下儿童和65岁以上老年人在个体化基础上经MDT讨论后确定药物治疗方案(本专家共识推荐强度:推荐) 定期监测米托坦引起的不良反应并予以适当治疗;为增加米托坦的耐受性,在严重不良反应发生前即开始支持性治疗(本专家共识推荐强度:强烈推荐) ENSAT:欧洲肾上腺肿瘤研究网;MDT:多学科诊疗;ACC:肾上腺皮质癌;TDM:治疗药物监测;CYP3A4:细胞色素P4503A4酶
下载: 导出CSV
表 3 2001年牛津循证医学中心推荐强度和证据等级分类
推荐强度 证据等级 描述 A 1a 同质随机对照试验的系统评价 1b 单项随机对照试验 1c “全或无”证据(有治疗以前,所有患者死亡;有治疗之后,有患者能存活。或者在有治疗之前,一些患者死亡;有治疗之后,无患者死亡) B 2a 同质队列研究的系统评价 2b 单项队列研究(包括低质量的随机对照试验,如<80%随访) 2c 结果研究,生态学研究 3a 同质病例对照研究的系统评价 3b 单项病例对照研究 C 4 病例报道(低质量队列研究) D 5 基于未经验证的专家意见或评论
下载: 导出CSV
表 4 晚期/复发性肾上腺皮质癌患者推荐治疗方案[13]
一线治疗方案 详细说明 米托坦(M)单药治疗 根据患者状况,采用低/高剂量起始方案,米托坦目标稳态血药浓度范围为14~20 mg/L EDP-M方案 40 mg/m2阿霉素(D),第1天;100 mg/m2依托泊苷(E),第2天;100 mg/m2依托泊苷(E)+40 mg/m2顺铂(P),第3~4天;同时口服米托坦(M), 目标稳态血药浓度范围为14~20 mg/L
每28天为1个治疗周期(E)P-M方案 100 mg/m2依托泊苷(E),第1天;100 mg/m2依托泊苷(E)+40 mg/m2顺铂(P),第2~3天;同时口服米托坦(M),目标稳态血药浓度范围为14~20 mg/L
每28天为1个治疗周期其他治疗选择 局部治疗 射频消融、化学栓塞、放疗等 吉西他滨+卡培他滨 吉西他滨800 mg/m2,第1、8天(每3周1次);卡培他滨口服,1500 mg/d,连续用药。根据个体情况,经MDT讨论后确定是否联合米托坦治疗 鼓励患者参加临床试验
下载: 导出CSV
表 6 易与米托坦发生相互作用的CYP3A4底物药物及其替代药物/方案[41]
适应证 CYP3A4底物药物 替代药物/方案 失眠 阿普唑仑,地西泮,咪达唑仑[47],佐匹克隆,唑吡坦 根据临床效应调整合用药物的剂量,必要时进行TDM 呕吐 部分5-羟色胺3受体拮抗剂:昂丹司琼,格拉司琼 甲氧氯普胺,苯海拉明 高血压 部分二氢吡啶类钙通道阻滞剂:氨氯地平,硝苯地平 ACE抑制剂;α-肾上腺素能受体拮抗剂;β-肾上腺素能受体拮抗剂;血管紧张素2拮抗剂;袢利尿剂;噻嗪类利尿剂 疼痛 部分阿片类药物:芬太尼,美沙酮,羟考酮,曲马多 吗啡,氢吗啡酮 心律失常 地尔硫卓 β-肾上腺素能受体拮抗剂 高胆固醇血症[49] 阿托伐他汀,洛伐他汀,辛伐他汀 普伐他汀,瑞舒伐他汀 感染(非典型病原体) 部分大环内酯类抗生素:红霉素,罗红霉素,克拉霉素 阿奇霉素,莫西沙星,环丙沙星 CYP3A4、TDM:同表 2;ACE:血管紧张素转化酶
下载: 导出CSV
-
[1] Kerkhofs TM, Verhoeven RH, Van JM, et al. Adren-ocortical carcinoma: a population-based study on incidence and survival in the Netherlands since 1993[J]. Eur J Cancer, 2013, 49: 2579-2586. doi: 10.1016/j.ejca.2013.02.034 [2] Kebebew E, Reiff E, Duh QY, et al. Extent of Disease at Presentation and Outcome for Adrenocortical Carcinoma: Have We Made Progress?[J]. World J Surg, 2006, 30: 872-878. doi: 10.1007/s00268-005-0329-x [3] Fassnacht M, Libe R, Kroiss M, et al. Adrenocortical carcinoma: a clinician's update[J]. Nat Rev Endocrinol, 2011, 7: 323-335. doi: 10.1038/nrendo.2010.235 [4] Fassnacht M, Terzolo M, Allolio B, et al. Combination Chemotherapy in Advanced Adrenocortical Carcinoma[J]. N Engl J Med, 2012, 366: 2189-2197. doi: 10.1056/NEJMoa1200966 [5] Hahner S, Fassnacht M. Mitotane for adrenocortical carcinoma treatment[J]. Curr Opin Investig Drugs, 2005, 6: 386-394. [6] Tang Y, Liu Z, Zou Z, et al. Benefits of Adjuvant Mitotane after Resection of Adrenocortical Carcinoma: A Systematic Review and Meta-Analysis[J]. Biomed Res Int, 2018, 2018: 9362108. [7] Libé R, Borget I, Ronchi CL, et al. Prognostic factors in stage Ⅲ-Ⅳ adrenocortical carcinomas (ACC): an European Network for the Study of Adrenal Tumor (ENSAT) study[J]. Ann Oncol, 2015, 26: 2119-2125. doi: 10.1093/annonc/mdv329 [8] Amini N, Margonis GA, Kim Y, et al. Curative Resection of Adrenocortical Carcinoma: Rates and Patterns of Postoperative Recurrence[J]. Ann Surg Oncol, 2016, 23: 126-133. doi: 10.1245/s10434-015-4810-y [9] Kerkhofs TM, Ettaieb MH, Hermsen IG, et al. Developing treatment for adrenocortical carcinoma[J]. Endocr Related Cancer, 2015, 22: R325-R338. doi: 10.1530/ERC-15-0318 [10] Hermsen I, Kerkhofs T, Butter C, et al. Surgery in adrenocortical carcinoma: Importance of national cooperation and centralized surgery[J]. Surgery, 2012, 152: 50-56. doi: 10.1016/j.surg.2012.02.005 [11] Terzolo M, Angeli A, Fassnacht M, et al. Adjuvant mitotane treatment for adrenocortical carcinoma[J]. N Engl J Med, 2007, 356: 2372-2380. doi: 10.1056/NEJMoa063360 [12] Fassnacht M, Assie G, Baudin E, et al. Adrenocortical carcinomas and malignant phaeochromocytomas: ESMO-EURACAN Clinical Practice Guidelines for diagnosis, treatment and follow-up[J]. Ann Oncol, 2020, 31: 1476-1490. doi: 10.1016/j.annonc.2020.08.2099 [13] Fassnacht M, Dekkers OM, Else T, et al. European Society of Endocrinology Clinical Practice Guidelines on the management of adrenocortical carcinoma in adults, in collaboration with the European Network for the Study of Adrenal Tumors[J]. Eur J Endocrinol, 2018, 179: G1-G46. doi: 10.1530/EJE-18-0608 [14] Nelson AF, Woodard G. Severe adrenal cortical atrophy (cytotoxic) and hepatic damage produced in dogs by feeding 2, 2-bis(parachlorophenyl)-1, 1-dichloroethane (DDD or TDE)[J]. Arch Pathol (Chic), 1949, 48: 387-394. [15] Bergenstal DM, Hertz RO, Lipsett MB, et al. Chemotherapy of adrenocortical cancer with o, p'DDD[J]. Ann Int Med, 1960, 53: 672-682. doi: 10.7326/0003-4819-53-4-672 [16] Terzolo M, Ardito A, Zaggia B, et al. Management of adjuvant mitotane therapy following resection of adrenal cancer[J]. Endocrine, 2012, 42: 521-525. doi: 10.1007/s12020-012-9719-7 [17] Shawa H, Deniz F, Bazerbashi H, et al. Mitotane-Induced Hyperlipidemia: A Retrospective Cohort Study[J]. Int J Endocrinol, 2013, 2013: 624962. [18] Weigand I, Schreiner J, Röhrig F, et al. Active steroid hormone synthesis renders adrenocortical cells highly susceptible to type Ⅱ ferroptosis induction[J]. Cell Death Dis, 2020, 11: 192. doi: 10.1038/s41419-020-2385-4 [19] Poli G, Guasti D, Rapizzi E, et al. Morphofunctional effects of mitotane on mitochondria in human adrenocortical cancer cells[J]. Endocr Relat Cancer, 2013, 20: 537-550. doi: 10.1530/ERC-13-0150 [20] LaPensee CR, Mann JE, Rainey WE, et al. ATR-101, a Selective and Potent Inhibitor of Acyl-CoA Acyltransferase 1, Induces Apoptosis in H295R Adrenocortical Cells and in the Adrenal Cortex of Dogs[J]. Endocrinology, 2016, 157: 1775-1788. doi: 10.1210/en.2015-2052 [21] Lin CW, Chang YH, Pu HF. Mitotane exhibits dual effects on steroidogenic enzymes gene transcription under basal and cAMP-stimulating microenvironments in NCI-H295 cells[J]. Toxicology, 2012, 298: 14-23. doi: 10.1016/j.tox.2012.04.007 [22] Zsippai A, Szabo DR, Tombol Z, et al. Effects of mitotane on gene expression in the adrenocortical cell line NCI-H295R: a microarray study[J]. Pharmacogenomics, 2012, 13: 1351-1361. doi: 10.2217/pgs.12.116 [23] Lehmann TP, Wrzesinski T, Jagodzinski PP. The effect of mitotane on viability, steroidogenesis and gene expression in NCIH295R adrenocortical cells[J]. Mol Med Rep, 2013, 7: 893-900. doi: 10.3892/mmr.2012.1244 [24] Bellantone R, Ferrante A, Boscherini M, et al. Role of reoperation in recurrence of adrenal cortical carcinoma: results from 188 cases collected in the Italian National Registry for Adrenal Cortical Carcinoma[J]. Surgery, 1997, 122: 1212-1218. doi: 10.1016/S0039-6060(97)90229-4 [25] Icard P, Goudet P, Charpenay C, et al. Adrenocortical carcinomas: surgical trends and results of a 253-patient series from the French Association of Endocrine Surgeons study group[J]. World J Surg, 2001, 25: 891-897. doi: 10.1007/s00268-001-0047-y [26] Calabrese A, Basile V, Puglisi S, et al. Adjuvant mitotane therapy is beneficial in non-metastatic adrenocortical carcinoma at high risk of recurrence[J]. Eur J Endocrinol, 2019, 180: 387-396. doi: 10.1530/EJE-18-0923 [27] Puglisi S, Calabrese A, Basile V, et al. Mitotane Concentrations Influence the Risk of Recurrence in Adrenocortical Carcinoma Patients on Adjuvant Treatment[J]. J Clin Med, 2019, 8: 1850. doi: 10.3390/jcm8111850 [28] Puglisi S, Calabrese A, Basile V, et al. Mitotane Concentrations Influence Outcome in Patients with Advanced Adrenocortical Carcinoma[J]. Cancers (Basel), 2020, 12: 740. doi: 10.3390/cancers12030740 [29] Gonzalez RJ, Tamm EP, Ng C, et al. Response to mitotane predicts outcome in patients with recurrent adrenal cortical carcinoma[J]. Surgery, 2007, 142: 867-875. doi: 10.1016/j.surg.2007.09.006 [30] Haak HR, Hermans JF, Lentjes EF, et al. Optimal treatment of adrenocortical carcinoma with mitotane: results in a consecutive series of 96 patients[J]. Br J Cancer, 1994, 69: 947-951. doi: 10.1038/bjc.1994.183 [31] Lagana M, Grisanti S, Cosentini D, et al. Efficacy of the EDP-M Scheme Plus Adjunctive Surgery in the Management of Patients with Advanced Adrenocortical Carcinoma: The Brescia Experience[J]. Cancers (Basel), 2020, 12: 941. doi: 10.3390/cancers12040941 [32] Williamson SK, Lew D, Miller GJ, et al. Phase Ⅱ evaluation of cisplatin and etoposide followed by mitotane at disease progression in patients with locally advanced or metastatic adrenocortical carcinoma: a Southwest Oncology Group Study[J]. Cancer, 2000, 88: 1159-1165. doi: 10.1002/(SICI)1097-0142(20000301)88:5<1159::AID-CNCR28>3.0.CO;2-R [33] Faggiano A, Leboulleux S, Young J, et al. Rapidly progressing high o, p'DDD doses shorten the time required to reach the therapeutic threshold with an acceptable tolerance: preliminary results[J]. Clin Endocrinol (Oxf), 2006, 64: 110-113. doi: 10.1111/j.1365-2265.2005.02403.x [34] Mauclere DS, Leboulleux S, Borget I, et al. High-dose mitotane strategy in adrenocortical carcinoma: prospective analysis of plasma mitotane measurement during the first 3 months of follow-up[J]. Eur J Endocrinol, 2012, 166: 261-268. doi: 10.1530/EJE-11-0557 [35] Terzolo MF, Daffara FF, Zaggia BF, et al. Management of adrenal cancer: a 2013 update[J]. J Endocrinol Invest, 2014, 37: 207-217. doi: 10.1007/s40618-013-0049-2 [36] Terzolo MB. Adjunctive treatment of adrenocortical carcino-ma[J]. Curr Opin Endocrinol Diabetes Obes, 2008, 15: 221-226. doi: 10.1097/MED.0b013e3282fdf4c0 [37] Kerkhofs T, Baudin E, Terzolo M, et al. Comparison of two mitotane starting dose regimens in patients with advanced adrenocortical carcinoma[J]. J Clin Endocrinol Metab, 2013, 98: 4759-4767. doi: 10.1210/jc.2013-2281 [38] Creemers SG, Hofland LJ, Feelders RA. Management of Adrenal Masses in Children and Adults[M]. Berlin, Germany: Springer International Publishing, 2017: 225-243. [39] Vezzosi DA, Do Cao C, Hescot S, et al. Time Until Partial Response in Metastatic Adrenocortical Carcinoma Long-Term Survivors[J]. Horm Cancer, 2018, 9: 62-69. doi: 10.1007/s12672-017-0313-6 [40] Reimondo G, Puglisi S, Zaggia B, et al. Effects of mitotane on the hypothalamic-pituitary-adrenal axis in patients with adrenocortical carcinoma[J]. Eur J Endocrinol, 2017, 177: 361-367. doi: 10.1530/EJE-17-0452 [41] Kerkhofs TM, Derijks LF, Ettaieb HF, et al. Development of a pharmacokinetic model of mitotane: toward personalized dosing in adrenocortical carcinoma[J]. Ther Drug Monit, 2016, 37: 58-65. [42] Bornstein SR, Allolio B, Arlt W, et al. Diagnosis and Treatment of Primary Adrenal Insufficiency: An Endocrine Society Clinical Practice Guideline[J]. J Clin Endocrinol Metab, 2016, 101: 364-389. doi: 10.1210/jc.2015-1710 [43] Daffara F, De Francia S, Reimondo GF, et al. Prospective evaluation of mitotane toxicity in adrenocortical cancer patients treated adjuvantly[J]. Endocr Relat Cancer, 2008, 15: 1043-1053. doi: 10.1677/ERC-08-0103 [44] Baudin E, Pellegriti GF, Bonnay MF, et al. Impact of monitoring plasma 1, 1-dichlorodiphenildichloroethane (o, p'DDD) levels on the treatment of patients with adreno-cortical carcinoma[J]. Cancer, 2001, 92: 1385-1392. doi: 10.1002/1097-0142(20010915)92:6<1385::AID-CNCR1461>3.0.CO;2-2 [45] Slooten H, Moolenaar A, Seters A, et al. The treatment of adrenocortical carcinoma with o, p'-DDD: prognostic implications of serum level monitoring[J]. Eur J Cancer Clin Oncol, 1984, 20: 47-53. doi: 10.1016/0277-5379(84)90033-6 [46] Terzolo M, Baudin AE, Ardito A, et al. Mitotane levels predict the outcome of patients with adrenocortical carcinoma treated adjuvantly following radical resection[J]. Eur J Endocrinol, 2013, 169: 263-270. doi: 10.1530/EJE-13-0242 [47] Erp NP, Guchelaar HJ, Ploeger BA, et al. Mitotane has a strong and a durable inducing effect on CYP3A4 activity[J]. Eur J Endocrinol, 2011, 164: 621-626. doi: 10.1530/EJE-10-0956 [48] Kroiss M, Quinkler M, Lutz WK, et al. Drug interactions with mitotane by induction of CYP3A4 metabolism in the clinical management of adrenocortical carcinoma[J]. Clin Endocrinol (Oxf), 2011, 75: 585-591. doi: 10.1111/j.1365-2265.2011.04214.x [49] Greenman Y. Management of dyslipidemia in Cushing's syndrome[J]. Neuroendocrinology, 2010, 92: 91-95. doi: 10.1159/000314294 [50] Tripto-Shkolnik L, Blumenfeld Z, Bronshtein M, et al. Pregnancy in a Patient With Adrenal Carcinoma Treated With Mitotane: A Case Report and Review of Literature[J]. J Clin Endocrinol Metab, 2013, 98: 443-447. doi: 10.1210/jc.2012-2839 [51] Corbière P, Ritzel K, Cazabat L, et al. Pregnancy in Women Previously Treated for an Adrenocortical Carcinoma[J]. J Clin Endocrinol Metab, 2015, 100: 4604-4611. doi: 10.1210/jc.2015-2341 [52] Rodriguez-Galindo C, Krailo MD, Pinto EM, et al. Treatment of Pediatric Adrenocortical Carcinoma With Surgery, Retroperitoneal Lymph Node Dissection, and Chemotherapy: The Children's Oncology Group ARAR0332 Protocol[J]. J Clini Oncol, 2021: 39: 2463-2473. [53] Liu X, Fu Q, Tang Y, et al. A case report of neurological adverse events caused by short-term and low-dose treatment of mitotane: The role of therapeutic drug monitoring[J]. Medicine (Baltimore), 2020, 99: e22620. doi: 10.1097/MD.0000000000022620 [54] Russo M, Scollo C, Pellegriti G, et al. Mitotane treatment in patients with adrenocortical cancer causes central hypothyroidism[J]. Clin Endocrinol (Oxf), 2016, 84: 614-619. doi: 10.1111/cen.12868 [55] Vikner ME, Krogh J, Daugaard G, et al. Metabolic and hormonal side effects of mitotane treatment for adrenocortical carcinoma: A retrospective study in 50 Danish patients[J]. Clin Endocrinol (Oxf), 2021, 94: 141-149. doi: 10.1111/cen.14345 [56] Tada H, Nohara AF, Kawashiri MF, et al. Marked transient hypercholesterolemia caused by low-dose mitotane as adjuvant chemotherapy for adrenocortical carcinoma[J]. J Atheroscler Thromb, 2014, 21: 1326-1329. doi: 10.5551/jat.27557 -

 点击查看大图
点击查看大图
图(1) / 表(6)
计量
- 文章访问数: 2895
- HTML全文浏览量: 332
- PDF下载量: 1583
- 被引次数: 0












